Abstract:
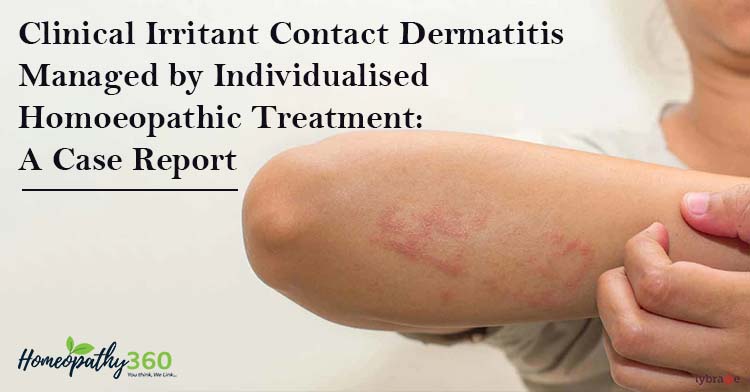
Irritant contact dermatitis is localised rash or irritation of skin caused by contact with a foreign substance. Irritant contact dermatitis occurs worldwide with an overall prevalence of 4% of some population. Many substances can cause this type of reaction but the commoner culprits are nickel (in costume jewellery and buckles); chromate (in cement); latex (in surgical gloves); perfume (in cosmetics and air fresheners); and plants (such as primula or composite). A good history is necessary and if suspicious, patch testing should be arranged to prove any allergy. Clinical experience and studies identify a positive role of homoeopathy in skin conditions including irritant contact dermatitis. This case treated with individualised homoeopathic medicine over a period of 3 month, shows significant improvement which is evident from the photographs. This case shows the usefulness of Homoeopathy in treating the irritant contact dermatitis.
Keywords: homoeopathy; irritant contact dermatitis; individualisation, Mercurius solubilis;
Abbreviation: contact dermatitis (CD)
Introduction:
Irritant contact dermatitis (CD) is an inflammatory reaction in the skin resulting from exposure to a substance that causes an eruption in most people who come in contact with it(1). Irritant contact dermatitis is a non-specific response of the skin to direct chemical damage that releases mediators of inflammation predominantly from epidermal cells while allergic contact dermatitis is a delayed (type 4) hypersensitivity reaction to exogenous contact antigens. Immunological responses are due to the interaction of cytokines and T cells. In photo contact, allergic dermatitis lesions are confined to sun-exposed areas even though the allergen is in contact with covered areas(2). Many substances act as irritants that produce a nonspecific inflammatory reaction of the skin. This type of dermatitis may be induced in any person if there is contact with a sufficiently high concentration. No previous exposure is necessary, and the effect is evident within minutes, or a few hours at most (3). Irritant CD is a non-specific skin response to direct chemical skin damage and/with releasing inflammatory mediators, while allergic CD is a delayed hypersensitivity reaction (type IV) to allergens, which includes immune responses (due to the interaction of T cells and cytokines (3).Irritant contact dermatitis can occur in any individual. It often occurs on the hands after repeated exposure to irritants such as detergents, soaps or bleach. It is therefore common in housewives, cleaners, hairdressers, mechanics and nurses. The concentration and type of toxic agent, duration of exposure, and condition of the skin at the time of exposure produce the variation in severity of dermatitis from person to person, or from time to time in the same person. Repeated exposure to some of the milder irritants may produce a hardening effect over time. This process makes the skin more resistant to the irritant effects of a given substance. Symptomatically, pain and burning are more common in irritant dermatitis, contrasting with the usual itch of allergic reactions (3).
The likelihood of developing irritant contact dermatitis (irritant contact dermatitis) increases with the duration, intensity, and concentration of the substance. Chemical or physical agents and microtrauma may produce skin irritation thus causing Irritant contact dermatitis. Physical irritants like friction, abrasions, occlusion, and detergents like sodium lauryl sulphate produce more irritant contact dermatitis in combination than alone. The factors which determine the severity of irritant contact dermatitis include the quantity and concentration of the irritant, duration, and frequency of exposure. It also depends on the type of skin if it is thick, thin, oily, dry, very fair, previously damaged skin, or having a pre-existing atopic tendency. Environmental factors like high or low temperature and humidity also determine the severity(4,5).
Females, infants, elderly, and individuals with atopic tendencies are more susceptible to irritant contact dermatitis. It is reported that up to 80% of cases of occupational dermatitis are irritant contact dermatitis. Data from the National Health Interview Survey (n = 30,074) showed a 12-month prevalence for occupational contact dermatitis of 1,700 per 100,000 workers. According to another study, the industries with the highest rates of contact dermatitis are natural resources and mining, manufacturing, and health services. Occupational skin diseases rank second only to traumatic injuries as the most common types of occupational disease. Chemical irritants, such as solvents and cutting fluids used in machining, account for most cases of irritant contact dermatitis. A study showed that hands were primarily affected in 64 percent of workers with allergic contact dermatitis and 80 percent of those with the irritant form(6).
When irritant CD lesions occur after exposure to a substance (even in small concentrations), effects may accumulate due to repeated influence commonly leading to chronic skin damages and skin lesions. Irritant CD may manifest in a form of acute and chronic lesions. There are many substances related to irritant CD, caused by their irritant or toxic effects, e.g., chemical agents, physical agents, plants, phototoxic agents, airborne irritants, etc (7). Chronic irritant CD may be induced by any substance causing acute irritant CD that, when in small concentrations, can accumulate effects causing chronic skin damages (even water, in cases of frequent hand washing, working in water, taking shower, bathing, etc. It is due to sufficient inflammation arising from the release of proinflammatory cytokines from keratinocytes, usually in response to chemical stimuli. It mainly causes skin barrier disruption, epidermal cellular changes, and cytokine release. Irritants can be classified as cumulatively toxic (e.g., hand soap causing irritant dermatitis in a hospital employee), subtoxic, degenerative, or toxic (e.g., hydrofluoric acid exposure at a chemical plant)(2).
Case study:
A 38 years old lady came to our outpatient department of Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, with complaints of severe itching, redness and burning sensation and scaly eruption in extensor surface of left hand and slight in right hand and in wave of digits of fingers for last 6 months. Her complaints were getting aggravated at night and from using any detergents, soaps, surgical gloves. Her complaints have started from the beginning of outbreak of Sars covid-19, she using in regular basic of sanitiser, hand wash, gloves, etc. After that for last 6 months her complaints have started and at first, she treated with modern medicine and local application of ointment, and complaint recurring again and again. As the disease progressed, the area became red with severe itching and burning at times, which became intolerable. History of past sufferings revealed that she has suffered from chicken pox at 9 years of age, history of suppression of skin eruption by local ointment, history of jaundice. Along with family history of bronchial asthma, type 2 diabetes mallitus, and hypertension of her father, Mother died of breast cancer. Among generals, her appetite was good, and could not tolerate hunger, takes water while eating. She had craving for sweets and cold drinks, also preferred fish, chicken, egg and sour food. Her thirst was intense for cold drinks although tongue looked moist. Her tongue was large with imprints of teeth. Her perspiration was profuse all over the body and complaints worsened during perspiration. She had an occasional history of dysenteric stool. She was sensitive both to heat and cold. She was introvert and always used to do everything in a hurried manner.
Analysis of the case:
With the help of characteristic mental and physical symptoms, the totality of symptoms was formed and individualisation of the case was done. Among physical general symptoms, her appetite was good, and could not tolerate hunger, takes water while eating. She had craving for sweets and cold drinks, also preferred fish, chicken, egg and sour food. Her thirst was intense for cold drinks although tongue looks moist. Her tongue was large with imprint of teeth. Her perspiration was profuse in all over the body and complaints worse during perspiration. She had an occasional history of dysenteric stool. She was sensitive to both heat and cold. She was introvert and always did everything in hurried manner. The totality of symptoms(8) helped to choose a medicine by considering the patient as a whole. After forming the totality, and confirmed by repertorial sheet and final selection was done after consulting with materia medica(9,10), the patient was prescribed Mercurius solubilis 30CH, 2 doses, and was instructed to take once in early morning in empty stomach followed by placebo for next 7 days. After taking medicine, her itching and redness subsided and returned to normal healthy skin.
Table 1: Repertorisation chart: (Kent Repertory was used as case had enough mental and physical generals)
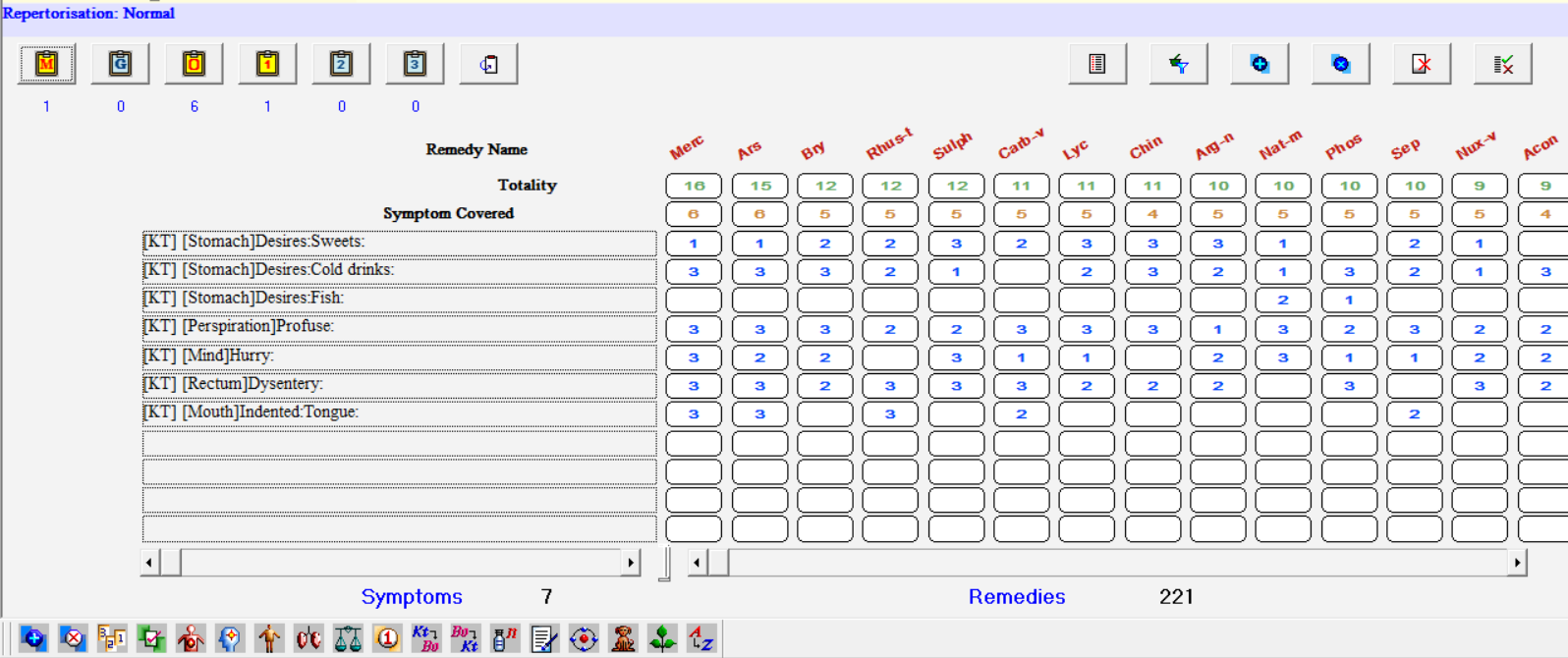
Table 2:
| Date | Presenting complaints | Medicine |
| First visit 19.05.20 | Severe itching, redness and burning sensation and scaly eruption in extensor surface of left hand. | Mercurius solubilis 30CH / 2dose, followed by placebo for 7 days. |
| Second visit 18.05.20 | Itching, redness and burning sensation and scaly eruption is subside. | Placebo for 15 days. |
| Third visit 1.06.20 | No itching, no eruption. | Placebo for 28 days. |
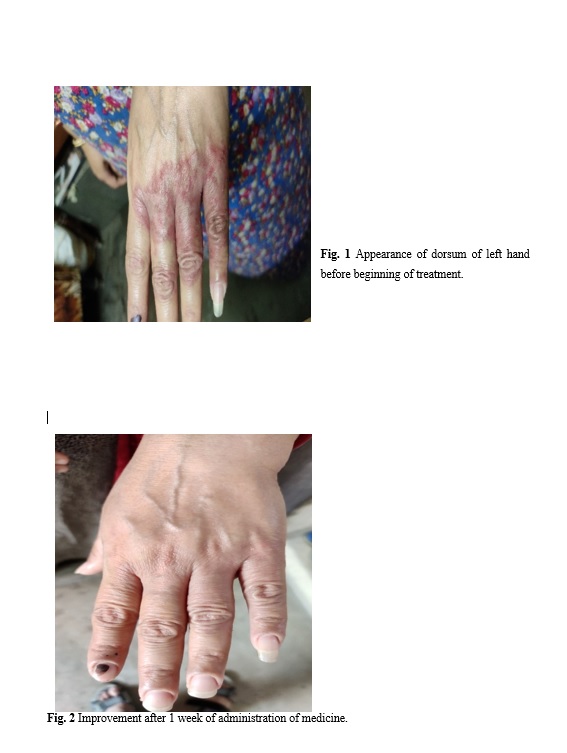
Fig. 1 Appearance of dorsum of left hand before beginning of treatment.
Fig. 2 Improvement after 1 week of administration of medicine.
Discussion:
Previously thought of as an immunologic inert process, at present, there is increasing evidence showing that irritant contact dermatitis is a complex, interlinked process involving perturbations in the skin barrier integrity, cellular changes, and release of various proinflammatory mediators(11–13). Homoeopathic treatment claims so because of its individualistic approach. Here in this case, a presentation of irritant contact dermatitis in the form of severe itching, redness and burning sensation and scaly eruption in extensor surface of left hand and slight in right hand and in wave of digits of fingers has been cured successfully with ultra-diluted homoeopathic medicines and medicine selection confirmed by the reportorial analysis by ‘Repertory of the Homeopathic Materia Medica by – J. T Kent(14), through Hompath Classic Software. It is true that exact mechanism of action is still unknown but that does not interfere with the acceptance of homoeopathy among the patient. In developing countries like India, disease complications are also associated with escalation in the cost of treatment, where homoeopathy can play a crucial role to cut down the cost of treatment as well.
Conclusion:
The above case report showed positive effect of treatment, individualised homoeopathic medicine in managing the irritant contact dermatitis.
Limitation of study:
As it is a single case report. In future case series can be recorded and published to establish the effectiveness of individualized homoeopathic medicine in irritant contact dermatitis.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent for treatment and publication of images without disclosing the identity of patient.
References:
1. Feather A, Randall D, Waterhouse M, Kumar PJ. Kumar & Clark’s clinical medicine. 2021.
2. Litchman G, Nair PA, Atwater AR, Bhutta BS. Contact Dermatitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [cited 2022 Feb 1]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK459230/
3. ROSENBACH. JAMES. TREAT. ANDREWS’ DISEASES OF THE SKIN: clinical dermatology. Place of publication not identified: ELSEVIER; 2019.
4. Bingham LJ, Tam MM, Palmer AM, Cahill JL, Nixon RL. Contact allergy and allergic contact dermatitis caused by lavender: A retrospective study from an Australian clinic. Contact Dermatitis [Internet]. 2019 Jul [cited 2021 Nov 21];81(1):37–42. Available from: https://onlinelibrary.wiley.com/doi/10.1111/cod.13247
5. Kimyon RS, Warshaw EM. Airborne Allergic Contact Dermatitis: Management and Responsible Allergens on the American Contact Dermatitis Society Core Series. Dermatitis [Internet]. 2019 Mar [cited 2021 Nov 21];30(2):106–15. Available from: https://journals.lww.com/01206501-201903000-00003
6. Usatine RP, Riojas M. Diagnosis and management of contact dermatitis. Am Fam Physician. 2010 Aug 1;82(3):249–55.
7. Novak-Bilić G. Irritant and Allergic Contact Dermatitis – Skin Lesion Characteristics. ACC [Internet]. 2018
; Available from: https://hrcak.srce.hr/index.php?show=clanak&id_clanak_jezik=317930
8. Hahnemann S, Boericke W, Dudgeon RE. Organon of medicine: word index included. New Delhi: B. Jain Publishers; 2011.
9. Allen HC. Keynotes and characteristics: with comparisons of some of the leading remedies of the materia medica with bowel nosodes. 2011.
10. Boericke W. Boericke’s new manual of homoeopathic materia medica with repertory: including Indian drugs, nosodes, uncommon rare remedies, mother tinctures, relationships, sides of the body, drug affinities, & list of abbreviations. New Delhi: B. Jain Publishers; 2007.
11. Lee HY, Stieger M, Yawalkar N, Kakeda M. Cytokines and chemokines in irritant contact dermatitis. Mediators Inflamm. 2013;2013:916497.
12. Smith HR, Basketter DA, McFadden JP. Irritant dermatitis, irritancy and its role in allergic contact dermatitis. Clin Exp Dermatol. 2002 Mar;27(2):138–46.
13. Lisby S, Baadsgaard O. Mechanisms of Irritant Contact Dermatitis. In: Frosch PJ, Menné T, Lepoittevin JP, editors. Contact Dermatitis [Internet]. Berlin/Heidelberg: Springer-Verlag; 2006 [cited 2022 May 29]. p. 69–82. Available from: http://link.springer.com/10.1007/3-540-31301-X_4
14. Kent JT, Kent CL. Repertory of the homeopathic materia medica. 2019.