Abstract:
“The obesity is definedas increase of the body weight 10-20% above the normal, which is caused by excessive accumulation of fat.” According to National Institutes of Health, Overweight and Obesity are defined on the basis of body mass index (BMI)—body weight in kilograms divided by height in square meters—because this measurement correlates strongly with total body fat content in adults. Obesity has been coexisted with increased coagulability, inflammation and endothelial dysfunction, as well as more prone to cardiovascular disease (CVD) risk factors such as insulin resistance and dyslipidemia consisting of hypertriglyceridemia. BMI and lipid parameters are favorable diagnostic criteria for to identify the hypercholesterolemic patient. Homoeopathy has been proved to be effective in the treatment of normalizing the altered lipid values and its symptoms in overweight and obese individuals, with homoeopathic specific remedy and modification of life style as well as proper diet can improve the patient quality of life.
Key words: Obesity, BMI, Hypercholesterolemia, Dyslipidemia
Introduction:
The term Obesity is derived from Latin word ‘Obesus’ which means ‘Stout or Plum’. Obesity is a term applied to excess body weight with an abnormally high proportion of body fat. Obesity acquired in childhood is a predictive factor of becoming obese in adulthood. World Health Organization used body mass index (BMI) to define severity of overweight and obesity across population. Accordingly, overweight is defined as a BMI of 25 to 29.9 and obesity as a BMI of ≥30. (1)
In India, more than 135 million individuals were affected by obesity. According to ICMR-INDIAB study 2015, prevalence rate of obesity and central obesity are varies from 11.8% to 31.3% and 16.9%–36.3% respectively in India. (2)
Obesity is associated with elevated blood lipids and lipoproteinsand high density lipoprotein estimation showed significantly decreased levels in obese. (3) Earlier research has shown that hypercholesterolemia increases predisposition to coronary heart disease (Rossouw, et ai, 1988). High levels of total serum cholesterol, and especially high levels of serum low-density lipoproteins (LDL) have been strongly indicated in atherosclerotic cardiovascular disease and Cerebrovascular ischemia & Framingham Heart Study also has been observed that obesity induces a several structural and functional alteration in cardiovascular systemand it’s confirmed that weight gain is associated with higher cholesterol levels and other factors like blood pressure, glucose and uric acid. (3)
Fat cells, residing within widely distributed adipose tissue deposits, are adopted to store excess efficiently as triglyceride and, when needed to release the stored energy as free fatty acids for use at other sites. This physiology system regulated through endocrine and neural pathway permits humans to survive from starvation for as long as several months.Declining physical activity, ingestion of foods high in fat and calories, increased the risk for development of obesity and related cardiovascular disease. (4)
Anthropometric Measurements: BMI= WIEGHT (Kg) / HIEGHT2 (METER)
Height, weight, waist, and hip were measured. Waist circumference (WC) =80-88 for women, 94-102 for men. Central obesity measured by the waist circumference (WC) and waist-to-hip ratio (WHR), have been as more accurate predictors of obesity-related cardiovascular risk. (5)
Classification of body weight according to BMI (6)
| Underweight BMI <18.5 kg/m2 |
| Normal or acceptable weight BMI 18.5–24.9 kg/m2 |
| Overweight BMI 25–29.9 kg/m2 |
| Obese BMI ≥30 kg/m2 |
| Grade 1 BMI 30–34.9 kg/m2 |
| Grade 2 BMI 35.0–39.9 kg/m2 |
| Grade 3 BMI ≥40 kg/m2 (severe, extreme, or morbid obesity) |
| Grade 4 BMI ≥50 kg/m2 |
| Grade 5 BMI ≥60 kg/m2 |
Abbreviations: BMI: Body mass index.
Epidemiology:
According to World Health Organization (WHO) 35% of adults aged >20 years were overweight (34% men and 35% women) in 2008 including 10% men and 14% women being considered as obese.Recent studies have reported that globally, more than 1.9 billion adults are overweight and 650 million are obese. Approximately 2.8 million deaths are reported as a result of being overweight or obese. (2)
General Classification:
- Primary hyperlipidaemia: in 1970s, Fredrickson and colleagues introduced of primary hyperlipidemia on bases of lipoprotein electrophoresis and ultracentrifugation. It’s also called familial hyperlipidemia due to genetic defect. (7)
Further classified into 3 groups (1)
| Class 1: in this type sr cholesterol level 280-400mmoI/l |
| Calss2: sr Triglyceride level is 200-499 mg/dl |
| Class3: deficiency of extra hepatic lipoprotein lipase. |
- Secondary hyperlipidaemia: this is acquired type of hyperlipidaemia; causes are drugs like corticosteroid’s, oral contraceptives, beta blockers, chronic alcoholics, diabetes. People prone to develop coronary, renal cerebral disease. (7,1)
Pathophysiology:
Fat is a biologically active tissue that produces chemical messengers (eg, adiponectin, resistin, angiotensin-2, tumor necrosis factor-α, and interleukins), (6) Leptin (adipose tissue) and Gherlin (stomach) are produced peripherally they control appetite through action on the central nervous system. When deficiency of leptin is leads to overfeeding and prone for the obesity. (8)
- Primary hypercholesterolemia caused by the defect in lipoprotein lipase activity, where lipid metabolism leads to a hypertriglyceridemia and hyper chylomicrons.(9)
- In secondary hypercholesterolemia pathology is depend on the underlying causes
In hypothyroidism the activity of low density lipoprotein and lipolytic activity will reduce the hepatic degradation of cholesterol to bile acids. (9)
- In cases of diabetes mellitus it’s noted that by liver high synthesis of low density lipoprotein will leads to hypercholesterolemia.
- In liver disease hypercholesterolemia has been noted to be caused by reduced excretion of cholesterol the bile.
Risk factors: (10, 11)
| Modifiable | Non – modifiable |
| Drugs ex: glucocorticoids, estrogens | Age, Gender |
| Obesity | Familial history of lipid disorder |
| Physical activity | Chronic disease ex: diabetes |
| Nutrition | Chronic alcoholism with increase plasma lipids |
Clinical features: (12)
Most of the times patient with high level of cholesterol will be asymptomatic, until laboratory investigation is detect.
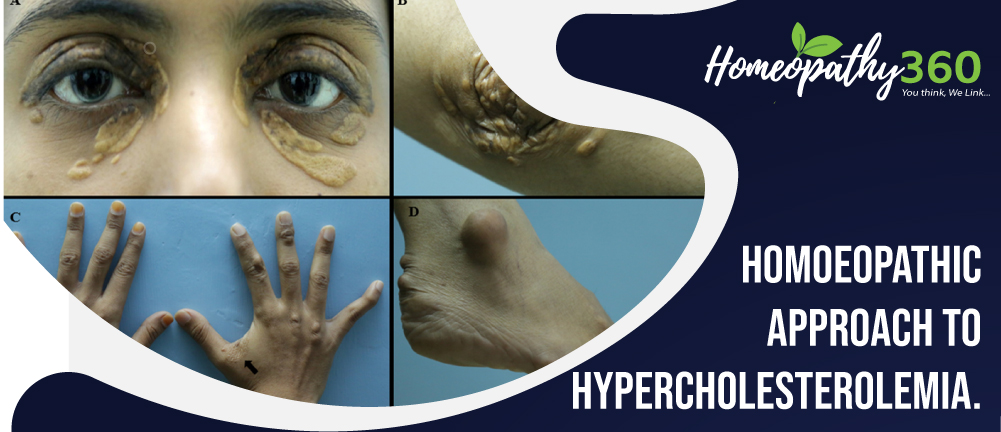
Genetic hyperlipidemia:
- Eruptive xanthomas: (sr triglyceride level id above 1000mg/dl) red, yellow papules especially on buttocks.
- Tendinous xanthomas: on certain tendons on patella, back of the hand (high level low density lipoprotein).
- Lipemia retinalis: cream colored blood vessels in fundus (high level of sr. triglyceride)
- Few already known symptoms are dyspnea, paraesthesia, and confusion.
Diagnostic criteria: (8)
National cholesterol education program recommended that fasting lipoprotein profile (FLP) should be measured in all adults 20 years of age or older at least every 5years.
- “Friedewald formula for low density of cholesterol”
- LDL-C = TC – HDLC – (TG/2.2) mmol/
LIPID PEOFILE PARAMETERS (13)
| Lipids | Desirable Value | Borderline | High Risk |
| Cholesterol | < 200 mg/dl | 200-239 mg/dl | 240 mg/dl |
| TGL | < 140 mg/dl | 150-199 mg/dl | 200-499 mg/dl |
| HDL | 60 mg/dl | 40-50 mg/dl | < 40 mg/dl |
| LDL | 60-130 mg/dl | 130-159 mg/dl | 160-189 mg/dl |
| Cholesterol /HDL ratio | 4.0 | 5.0 | 6.0 |
Complication:
- Stroke
- Atherosclerosis
- Heart attack
- Diabetes mellitus (3,4)
General management (1, 2, 4)
With drug therapy alone it’s not possible to prevent the complication of hypercholesterolemia life style modification is also important.
- Dietary: moving from saturated animal fats to understand vegetable oil based fats.
- Physical activity
- Maintaining normal body weight (BMI 18 – 25)
- Weight reeducation
- Food to be avoided – sweet items, pastries, ice creams, jam, jellies, bakery products
The recent studies have shown that low carbohydrate diets are as effective as low fat diet for weight loss.
Homoeopathic management: (14, 15, 16)
Homoeopathy has been proved to be effective in the treatment of normalizing the altered lipid values and its symptoms in hypercholesterolemic, if any; it also helps in preventing the recurrence and being obese. With homoeopathic specific remedy and modification of life style as well as proper diet can improve the patient quality of life.
Alium sativa:
- Voracious diet, desire for butter.
- Suited to fleshy people and those used to high living, fleshy person, whose bowels deranged by the least irregularity of diet.
Alumina:
- Alumina is suited to person of sedentary habits who suffer from chronic ailments to constitution with diminished animal heat.
- Appetite bulimia irregular appetite, at one time too strong at another too week.
- Craving for starch, chalk, charcoal, cloves. Coffee or tea ground, indigestible things.
Ammonium muriaticum:
- Especially to those who are fat and sluggish or body large and fat but legs too thin.
- Obstinate constipation accompanied by much flatus expulsion crumbles from the verge of anus.
Antimonium crud:
- For children and young people inclined to grow fat.
- Old people with morning diarrhea, suddenly become constipated, or alternate diarrhoea and constipation.
Arum metallicum:
- Obesity in elderly people.
- Ailments from grief, fright, anger, mortification.
- Profound states of melancholy and depression.
- No love of life.
Belladonna:
- Large, fat people, bloated.
- Obesity in children.
- Obesity always associated with hot, flushed face, glaring eyes, throbbing carotids, excited mental state.
- Indicated for those people who are internally very weak but obese.
- Bulimia, with sickly taste in mouth.
Ferrum metallicum
- Obesity with anaemia, puffiness of face with pitting of flesh.
- Best adapted to young weak persons, anaemic and chlorotic with pseudo plethora that has cold extremities.
Fucus vesiculosis
- Best remedy for anti-obesity and nontoxic goitre.
- Digestion is improved and flatulence diminished.
- Obstinate constipation.
- Thyroid enlargement in obese people.
Graphitis
- Tendency to obesity in females with delayed menstruation.
- Patients are stout, fair complexion, prone to skin affections and constipation.
- Take cold easily.
Iodum
- Appetite variable, bulimia, absence of appetite, unusual hunger with amelioration after a meal.
- Eat too often and too much.
- Rapid digestion.
Iodothyrine
- Reducing weight may produce glycosuria.
- Use cautiously in obesity for a fatty heart may not be able to maintain accelerated rhythm.
Phytolacca
- Reduce the fat thus reduce the weight.
- Glandular remedy.
- General soreness, lameness, bruised feeling over whole body.
- Glands are swollen, heat and inflammation.
Piper nigra
- Disposition of abdomen and chest to obesity.
- Abdomen swollen, hard, burning.
Natrum muriaticum
- Weight gain is due to continued stress or depression.
- Dislike to food, especially when fat.
- Bulimia without appetite.
- Fullness sensation, craving for salt.
Lycopodium
- Upper part is wasted; lower part of the body is semi dropsically.
- Accumulation of excess fat over thighs and buttocks.
- Craving for sweet, bulimia.
- Tendency to eat far beyond the capacity.
Senega
- Especially suited for person of lax fibres who tend to become obese and for children who are chubby in appearance.
Sepia
- Obesity in females with weakness, yellow complexion and bearing down sensation.
- Obesity in menopausal women with hot flushes and perspiration.
- Sensitive to cold air, lack of vital heat especially in chronic disease.
List of reference’s
- krishnadas k. Text Book of Medicine. 5th ed. Delhi: Jaypee Brothers; 2014. pp.168-171.
- Ahirwar R, Mondal PR. Prevalence of Obesity in India: A systematic review. Diabetes Metab Syndr. 2019Jan-Feb:13 (1):318-321. doi: 10.1016/j.dsx.2018.08.032. Epub 2018 Sep 21. PMID: 30641719.
- Bhatti MS, Akbri MZ, Shakoor M. Lipid profile in obesity. Journal of Ayub Medical College Abbottabad. 2001;13(1):31-3
- Hasuer, Longo Jameson, Loscalzo, F. B. K Harrison’s internal Medicine. 17th ed. New york,; 2018. Pp.462-463.
- Wang T, Jónsdóttir R, Liu H, Gu L, Kristinsson HG, Raghavan S, Ólafsdóttir G. Antioxidant capacities of phlorotannins extracted from the brown algae Fucus vesiculosus. Journal of agricultural and food chemistry. 2012 Jun 13;60(23):5874-83
- Sowers JR. Obesity as a cardiovascular risk factor. Am J Med. 2003 Dec 8;115(8, Supplement 1):37–41.
- Shattat G. A Review Article on Hyperlipidemia: Types, Treatments and New Drug Targets. Biomedical and Pharmacology Journal. 2014;7(2):399-409.Lk
- .Hasuer, Longo Jameson, Loscalzo, F. B. K Harrison’s internal Medicine. 17th ed. New york,; 2018. Pp.462-463.
- Onwe PE, Folawiyo MA, Anyigor-Ogah CS, Umahi G, Okorocha AE, Afoke AO. Hyperlipidemia: etiology and possible control. IOSR J Dent Med Sci. 2015;14(10):2279-861.
- Nouh F, Omar M, Younis M. Risk Factors and Management of Hyperlipidemia (Review). AJCR [Internet]. 29Dec.2018 [cited 18Mar.2022];2(1):1-0. Available from: https://www.journalajcr.com/index.php/AJCR/article/view/29680
- Ballinger A. Essentials of Kumar and Clark’s Clinical Medicine E-Book. Elsevier Health Sciences; 2011 Sep 29.
- McPhee SJ, Papadakis MA, Rabow MW, editors. Current medical diagnosis & treatment 2010. New York:: McGraw-Hill Medical; 2010 Nov 5.
- Verma, Niharika. Introduction to hyperlipidemia and its treatment: a review. Int J Curr Pharm Res 2017;9(1):p.6-14; (Accessed on 1st March 2019) .
- Boericke W. Materia medica with repertory. InMateria medica with repertory 1927 (pp. 1049-1049).
- Kent JT. Repertory of the homoeopathic materia medica. B. Jain Publishers; 1992.
- Allen TF. A handbook of materia medica and homoeopathic therapeutics. FE Boericke; 1889
About Author:
Dr Hanamanth
Md Part-1
Deptment of Practice of Medicine
Father Muller Homoeopathic Medical College and Hospital Mangaluru -575018