ABSTRACT
Attention deficit hyperactive disorder is the most common neuro behavioral disorder, among the most prevalent chronic health conditions affecting school-aged children, and the most extensively studied mental disorder of childhood. ADHD is characterised by inattention, including increased distractibility and difficulty sustaining attention; poor impulse control and decreased self-inhibitory capacity; and motor over activity and motor restlessness.
KEY WORDS: ADHD, homoeopathy.
ABBREVIATIONS: ADHD – attention deficit hyperactive disorder; DAT 1 – dopamine active transporter; DRD 4 -dopa responsive dystonia; AF-after food; BF- before food; DSM-diagnostic and statistical manual of mental disorders; USA-united states of america; IQ- intelligent quotient
INTRODUCTION
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurobehavioral disorder of childhood, among the most prevalent chronic health conditions affecting school-aged children, and the most extensively studied mental disorder of childhood. ADHD is characterised by inattention, including increased distractibility and difficulty sustaining attention; poor impulse control and decreased self-inhibitory capacity; and motor over activity and motor restlessness.[1]
The simplest way to conceptualise a psychiatric disorder is a disturbance of cognition (i.e. thought), cognation (i.e. action), or affect (i.e. feeling), or any disequilibrium between the three domains. 1]
Characteristics of ADHD include poor selective attention, difficulty focusing, or distractibility. Hyperactivity may or may not be present. Attention deficit hyperactivity disorder (ADHD) it is defined as hyperactivity, impulsiveness and inattentiveness inappropriate for age. Boys suffer thrice compared to girls.[2]
Children with disorders of attention may show impulsivity, distractibility, disinhibition, and general behavioral immaturity[3].
Disorder is characterised by attention deficit, hyperactivity and impulsiveness for6 months which causes moderate psychological, social and/or educational impairment in 2 important settings (home, school, peers). [4]
AETIOLOGY
No single factor determines the expression of ADHD; mothers of children with ADHD are more likely to experience birth complications, such as toxemia, lengthy labour, and complicated delivery. Maternal smoking and alcohol use during pregnancy and prenatal or postnatal exposure to lead are commonly linked to attentional difficulties associated with the development of ADHD. Food colorings and preservatives have inconsistently been associated with hyperactivity in previously hyperactive children. [5]
There is a strong genetic component to ADHD. Genetic studies have primarily implicated 2 candidate genes, the dopamine transporter gene (DAT1) and a particular form of the dopamine 4 receptor gene (DRD4), in the development of ADHD.[5]
Abnormal brain structures are linked to an increased risk of ADHD; 20% of children with severe traumatic brain injury are reported to have subsequent onset of substantial symptoms of impulsivity and inattention. These include dysregulation of the frontal subcortical circuits, small cortical volumes in this region, widespread small-volume reduction throughout the brain, and abnormalities of the cerebellum. [5]
INCIDENCE
ADHD affects 3 to 4 percent of children in the USA. Boys are more affected than girls in a 6:1 ratio. ADHD persists into adolescence and adult life. Age of onset is usually before 4 years but diagnosis is made around 3 to 4 years of age. Statistical data is not available for the Indian children; experts agree that it is roughly the same percentage as in the western population.[6]
CLINICAL FEATURES
- Symptoms of inattention, including not being able to focus during classroom instruction, difficulty with organization, and forgetfulness
- Symptoms of hyperactivity, which may include fidgeting, acting as if driven by a motor, excessive talking, and difficulty remaining seated in the classroom
- Symptoms of impulsivity, which may include behavior such as blurting out answers before a question is completed
- Effect of attention problems on the child with ADHD Difficulty conforming to classroom routine
Development of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria leading to the diagnosis of ADHD has occurred mainly in field trials with children 5-12 year of age . The current DSM-IV criteria state that the behaviour must be developmentally inappropriate (substantially different from that of other children of the same age and developmental level), must begin before 7 year of age, must be present for at least 6 months, must be present in 2 or more settings, and must not be secondary to another disorder. DSM-IV identifies 3 subtypes of ADHD. [7]
The 1st subtype
Attention-deficit/hyperactivity disorder, predominantly inattentive type, often includes cognitive impairment and is more common in females. [7]
The 2nd subtype
- Attention- deficit/hyperactivity disorder, predominantly hyperactive-impulsive type, and attention deficit/hyperactivity disorder, combined type, are more commonly diagnosed in males.
DIAGNOSIS:
The diagnosis of ADHD is based on the criteria of DSM IV on hyperactivity, impulsivity and attention deficit. Psychometric tests should cover four essential areas— language skills, visuospatial skills, sequential analytic skills and motor planning and execution skills. Educational level, as measured on the peabody individual achievement test and the wide range achievement test, may be lower than expected for age IQ, especially for children who also have learning disabilities. Specific test for learning disabilities should be administered to pin point areas of difficulty. [8] (at least six of the following criteria for a minimal of six months)
- Inattention: often fails to give close attention to details or makes careless mistakes in school work or other activities.
- Often has difficulty in sustaining attention in takes or play activity.
- Often doesn’t seem to listen where spoken to directly.
- Often doesn’t follow through instructions and fails to finish schoolwork, chores, and duties in workplace.
- Often has difficulty in organising tasks and activities.
- Often avoids, dislike, or is reluctant to engage in tasks that require sustained mental effort.
- Often loses things necessary for talks or activities, for example toys, school assignments, pencils, books, tools.
- Often easily distracted by extraneous stimuli.
- Often forgetful in daily activities.
TREATMENT INTERVENTION
FOR BEHAVIOURAL PROBLEMS
For kids whose impulsive behaviour is creating conflict at home and getting them into trouble at school, therapy can help them rein in the behaviour that’s problematic and establish more positive relationships with the adults in their lives. It trains parents to interact differently with children, in order to elicit desirable behaviour on the part of the child and discourage behaviour that’s causing him trouble.[9]
They result in better behavior on the part of children, decreased arguing and tantrums, better parent-child interactions, and reduced parental stress.[9]
SCHOOL INTERVENTION
Young children with ADHD can benefit from systems that encourage positive behaviour, like the “daily report card.” These approaches pinpoint specific goals for behaviour in school, give kids feedback on how they’re doing, and reward them for meeting those goals successfully.[9]
FOR ATTENTION PROBLEMS:
The other broad area of behavioural help for kids with ADHD includes skills-based interventions to teach techniques they can use to stay on top of their schoolwork and manage their responsibilities at home. This kind of training, which is done by learning specialists, teaches kids skills to maximize their strengths and compensate for their weaknesses.[9]
INVESTIGATION
Scoring the Vanderbilt ADHD diagnostic rating scale
Scoring the Conner’s comprehensive behavior rating scale [10]
- SOME RUBRICS IN THE KENT’S REPERTORY WHICH HAS BEEN TAKEN FOR THE ADHD REFERENCES ARE[11];
- ABSENT MINDED -MIND CHAPTER
- ABSORBED, buried in thought – MIND CHAPTER
- ABUSIVE – MIND CHAPTER
- AGITATION – MIND CHAPTER
- , excitable
- AMOROUS : (see lewdness and lascivious, also genitalia)
- ANGER , irascibility (see irritability and quarrelsome)
- ANTICIPATION, complaints from
- ANXIETY
- ATTENTION (see concentration)
- BITING
- BUFFOONERY
- behavior(see childish)
- CAPRICIOUSNESS
- CARELESS HEEDLESS
- CLINGING to persons or furniture
- COMPREHENSION ,DULLNESS, morning, rising, on
- CONFUSION of mind
- DELUSIONS, imaginations, hallucinations, illusions
- DESTRUCTIVENESS
- DISOBEDIENCE
- DULLNESS, sluggishness, difficulty of thinking and comprehending
- FORGETFUL (see memory)
- GESTURES, makes
- LASCIVIOUSNESS, lustful
- LAUGHING
- MEMORY, weakness of weakness of (see mistakes)
Case presentation:
Mast. X of age 5 came with the complaint of hyperactivity, with poor concentration, irritability, shouting, inability to speak two words together at a same time since one year. The patient also has the habit of biting things, gets anger very easily when things not offered and doesn’t obey to whatever told. He easily forgets names and places. Birth history reveals the mother had threatened abortion in her first pregnancy 7 years back. This is her second pregnancy and she did not have any complications.
Physical Generals
Patient has a good appetite of having three meals per day with an average thirst of 1.5 litres of water per day. Patient had desire forsweets +++. Bowel habits were regular once a day without no discomfort. Passed urine 4-5 times per day. Sleep was disturbed due to complaints.
Analysis and evaluation of symptoms
| Mental generals | Physical generals | Particulars |
| Irritable++ (psora) Poor concentration(psora) Difficulty in speaking two words together(psora) Forgetful (sycosis) Didn’t obey (psora) Shouting (syphilis) Anger++ (psora) | Desire – sweets+++ (psora) Sleep – disturbed (psora) | _____ |
Fig 1: Hompath Zomoeo Sheet[12]
REPERTORIAL RESULT:
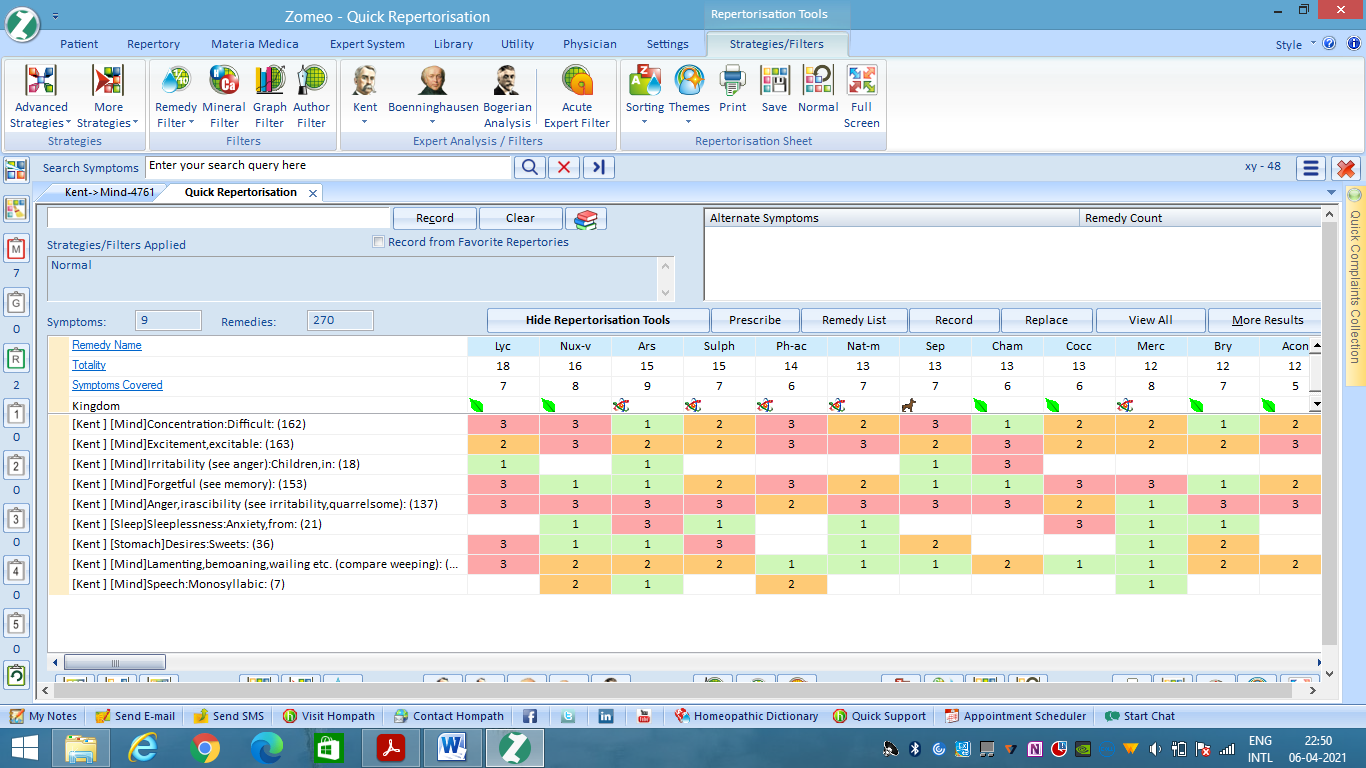
Prescription:
Arsenicum album 200 /1 dose
(anger excited easily; restlessness; irritable; lamenting; poor memory; sleep disturbed; lack of concentration; poor memory) (13)
(Potency and dosage – twelfth to thirtieth, higher and in infrequent dosage)(13)
Placebo(4-0-4) / 15 days, AF
Follow up –
| S.No. | SYMPTOMS | PRESCRIPTION |
| 1. | Patient felt better. Anger slightly reduced. Sleep improved. | Arsenicum album 200/ 1 dose. (every correctly chosen homoeopathic medicine, even those whose action is of long duration, may be repeated daily for months with ever increasing success – § 248) [ 14] Placebo (3- 0 – 3) AF/ 15 days |
| 2. | Patient felt better. 30% improvement. Anger slightly reduced. Sleep improved. Concentration slightly improved. | Placebo (3-0-3)/ 15 days, AF |
| 3. | Patient felt better. Generals were good. Aggressiveness reduced. Sleep improved. | Placebo (3-0-3) AF/ 15 days |
| 4. | Patient felt better with all complaints. Generals good. No new complaints. | Placebo (3-0-3) AF/ 15 days. |
CONCLUSION:
Homoeopathy has a very positive effective in all stages of ADHD. Individualised homoeopathic medicines based on constitutional remedies does wonders in the treatment of ADHD. It helps arrest further progress of disease and hence deterioration caused by disease.
REFERENCES:
- Richard E. Behrman, MD, Robert M. Kliegman, MD, Hal B. Jenson, MD. Nelson textbook of paediatrics.19thed.Netherlands: Elsevier publications;2011.P 3, 5, 6, 7, 8,9.
- Niraj Ahuja.A short textbook of psychiatry.7thed.New Delhi:Jaypee Brothers Medical Publishers (P) Ltd;2011. P 3
- Suraj Gupte. The short book of paediatrics. 11thed.New Delhi: Jaypee Brothers Medical Publishers (P) Ltd ;2009.P 3, 6, 10,
- Lloyd J.Brown, Ryan J.Coller,Lee Todd Miller.BRS paediatrics.2nded.Lippincott Williams and Wilkins; 2005. P 5, 6, 11
- Helen A. Brough, Ram Natraja.Rapid paediatrics and child health. 2nded.Oxford , U.K Hoboken , N.J Wiley – Blackwell;2010. P 6
- A.Parthasarathy. IAP textbook of paediatrics. 4thed. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd ;2009.P 6, 8, 9
- Vinod K Paul, Arvind Bagga.O P Ghai essential paediatrics. 8thed .CBS Publishers & distributors;2013. P 10, 11
- Krishna M Goel, Devendra K Gupta. Hutchison’s paediatrics. 2 nded. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd ;2012. P 12
- American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Association: Arlington, VA, ISBN 9780890425572
- Volkow ND, et al. (2009). Evaluating dopamine reward pathway in ADHD: Clinical implications. DOI:10.1001/jama.2009.1308
- J.T.Kent.Kent’s repertory of the homoeopathic materia medica.Reprint edition.New Delhi: B.Jain Publishers(p) ltd;p 20, 21, 22, 23,24,25,26,
- Hompath Zomoeo Software
- Boericke’s New manual of Homoeopathic Materia Medica with Repertory, William Boericke, third revised & augmented edition based on ninth edition, B.Jain publishers, New Delhi.
- Organon of Medicine, Dr. Samuel Hahnemann, VI edition, B.Jain publishers, New Delhi.
About the authors:
Dr J. Senthilkumar, B.H.M.S, M.D (HOM), Professor, PG Guide, Head of
Department, Department of Repertory, Vinayaka Mission’s Homoeopathic
Medical College & Hospital, A Constituent college of VMRF- Deemed to be
University, Salem, Tamil nadu.
Dr R.Sri Vaishnavi, Assistant Professor, Department of Repertory, Vinayaka Mission’s Homoeopathic Medical College & Hospital, A Constituent college of VMRF- Deemed to be University, Salem, Tamil nadu.
Dr A.M. Aarthi, B.H.M.S, Post Graduate Student, Department of Repertory,
Vinayaka Mission’s Homoeopathic Medical College & Hospital, A Constituent
college of VMRF-Deemed to be University, Salem, Tamil nadu