ABSTRACT: Essential hypertension (also known as primary or idiopathic hypertension) is defined as high blood pressure in the absence of any other identifiable secondary cause. In spite of medical advances, essential hypertension remains a major modifiable risk factor for renal and cardiovascular disorders.
The case study presented is of a 27-year old man, a diagnosed case of essential hypertension successfully treated with individualised homoeopathy. Majority of the presenting symptoms were common to the disease yet sufficient characteristic symptoms were elicited to enable the choice of simillimum. This case aptly illustrates the role of individualised homoeopathic treatment along with lifestyle correction to halt and reverse the progression of essential hypertension.
ABBRIEVIATIONS: BP– Blood pressure, mm of Hg- millimetre of mercury, OD –once a day, HS-at bedtime, SL – Saccharum lactis, Adv- advised
INTRODUCTION: Essential hypertension accounts for 95% of all cases of hypertension.1
AETIOLOGY: Although it has frequently been indicated that the causes of essential hypertension are not known, this is only partially true as one haa a little information on genetic variations or genes that are overexpressed or under expressed as well as the intermediary phenotypes that they regulate to cause high BP1
PATHOPHYSIOLOGY: The pathogenesis of essential hypertension is multifactorial and complex. Multiple factors modulate the blood pressure (BP) including humoral mediators, vascular reactivity, circulating blood volume, vascular calibre, blood viscosity, cardiac output, blood vessel elasticity, and neural stimulation. A possible pathogenesis of essential hypertension has been proposed in which multiple factors, including genetic predisposition, excess dietary salt intake, and adrenergic tone, may interact to produce hypertension. Although genetics appears to contribute, the exact mechanisms underlying essential hypertension have not been established.2
PROGRESSION: The progression of essential hypertension is as follows:
- Prehypertension in persons aged 10-30 years (by increased cardiac output)
- Early hypertension in persons aged 20-40 years (in which increased peripheral resistance is prominent)
- Established hypertension in persons aged 30-50 years
- Complicated hypertension in persons aged 40-60 years2
FACTORS THAT MODIFY THE COURSE OF ESSENTIAL HYPERTENSION3
- Age : Younger the patient when hypertension is first noted, greater is the reduction in life expectancy if the elevated blood pressure is left untreated
- Race : In the United States, those with black ancestry have twice the prevalence of hypertension as compared to the whites
- Sex: Females with elevated blood pressure fare well than males upto 65 years of age
- Obesity : There is a positive correlation between weight gain and development of hypertension
Hypertension is mostly accompanied by accelerated atherosclerosis. Hence, independent risk factors associated with the development of atherosclerosis like cigarette smoking, glucose intolerance and/or elevated serum cholesterol levels significantly magnify the effect of elevated blood pressure on the mortality rate, irrespective of sex, age, or race.
SIGNS AND SYMPTOMS: In most cases, there will be no apparent symptoms of essential hypertension, and it will only be discovered during a regular medical examination. A strong family history of increased blood pressure along with reported findings of intermittent increase in pressure in the past, favours a diagnosis of essential hypertension.
Other symptoms that may be related to elevated blood pressure are:
- Dizziness
- Palpitation
- Headache
- Easy fatigability
- Impotence
If essential hypertension is not diagnosed, the condition has the potential to worsen and create heart or kidney problems.4
TREATMENT
The main goal of treatment is to prevent end organ damage and decrease the risk of mortality. Most adults with untreated hypertension develop increased arterial pressure over time. Even in its mildest form (i.e. with no evidence of any end organ damage), if hypertension is left untreated for 7-10 years, there is a high risk of developing significant complications.3
Homoeopathy seeks to address the root cause of the high blood pressure whether at mental, emotional, physical or environmental levels. The following is a documented case demonstrating the potential role of homoeopathy as an effective treatment modality for a pathological condition like essential hypertension.
CASE STUDY
A 27-year old single male, resident of Mumbai, reported to the clinic on 30/10/2017, with frequent episodes of mild headache since December 2016. He had already been to a general physician and was diagnosed to be having essential hypertension (blood pressure was 140/90 mm of Hg) for which he was put on anti-hypertensives (tablet telma 40 -1 OD and tablet amlong 2.5 -1HS ) since January 2017. Even with this treatment, the frequency and intensity of headaches was persistent.
| LOCATION | SENSATION | MODALITIES | CONCOMITANT |
| FACE (forehead) | Dull, heavy headache with occasional vertigo | Better temporarily by lying down | Constipation |
ASSOCIATED COMPLAINTS:
- Recurrent upper respiratory tract infection (has this complaint since childhood)-blocked sensation in the nostrils only at night
- Premature greying of hair – since age of 20 years, but has increased since the past 6 months
PAST HISTORY:
- Repeated episodes of sneezing, cold and nasal obstruction. Diagnosed as deviated nasal septum, was advised surgery (sub mucous resection). Patient did not undergo it so far.
FAMILY HISTORY:
- Mother – 50 years old. Hypertension and osteoarthritis (on medication for both)
- Father – 54 years old. Had a paralytic attack 2 years back. Recovered fully.
- Elder sister – 34 years old, no significant health history.
- Maternal uncle – hypertension – on medication.
PHYSICAL GENERALS: Patient’s appetite, thirst, stool and urine were normal. Perspiration was moderate. Patient had a strong craving for sweets and rice.
Thermal state- Chilly (cannot tolerate cold weather or air conditioner at all. Desired for warmth in all seasons)
MENTAL GENERALS: Patient said that earlier he was short tempered but has calmed down since he has started this course of meditation. When asked about how he feels about taking anti hypertensives at such a young age, he said that it makes no difference to him. He has come for treatment only because his family coerced him.
LIFE SPACE: Patient used to stay with his parents. His father lost his job when the patient was around 15 years of age. Since then, he started doing odd jobs with his mother to improve the family’s financial condition. He had come up a very hard way and had to struggle for his education.
(Observation – When the patient narrated this history, his face was devoid of any expression or reaction. He was very matter of fact and showed very little expression when narrating his difficult and his physical complaints too)
DIAGNOSIS ANALYSIS:
1. Clinical diagnosis – essential hypertension
2. ICD-10-CM diagnosis code I10 5
| SYMPTOM | TYPE | INTENSITY (on a scale of 1 to 5 |
| Fearless | Characteristic mental symptom | 5+ |
| Stoic nature | Characteristic mental symptom | 5+ |
| Chilly | Characteristic physical general symptom | 5+ |
| Lack of reaction | Characteristic physical general symptom | 5+ |
| Desire for sweets | Characteristic physical general symptom | 5+ |
| Desire for rice | Characteristic physical general symptom | 5+ |
RUBRICS CHOSEN AFTER CASE ANALYSIS
- Mind- Fearless
- Mind-Indifference-stoical to what happens
- Mind-responsibility-early-taking responsibility too
- Generals-Food and drinks-rice desire
- Generals-Food and drinks-sweets desire
- Generals-Heat-lack of vital heat
- Generals-reaction lack of
REPERTORISATION 6
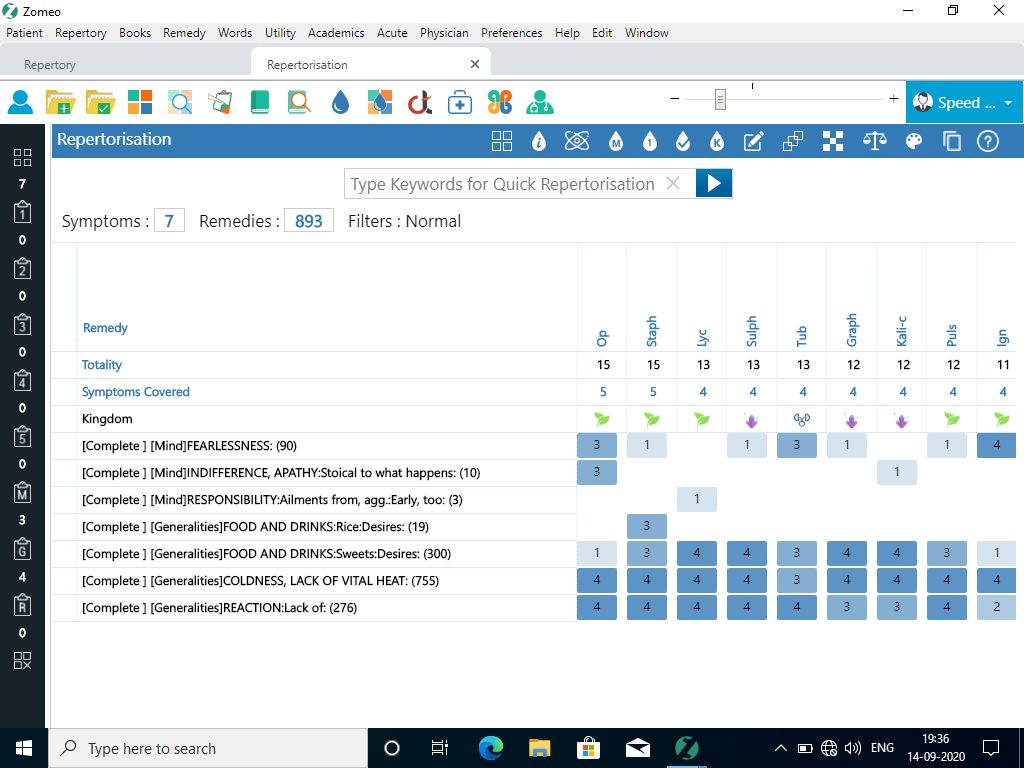
REMEDY ANALYSIS AND DISCUSSION:
After repertorisation, the main remedies that came out included Opium (15/5), Staphysagria (15/5) and Lycopodium clavatum (15/4),
Staphysagria came close to Opium after repertorisation but it didn’t cover the state of indifference.
REMEDY JUSTIFICATION
Opium covers all the physical symptoms as well the mental and emotional state of the patient. Lack of reaction is the core of this patient.
An Opium patient is unable to understand or appreciate his sufferings .7 Many Opium provers taking small doses had torpor, inability to realise or feel their surroundings, or to take in the nature of states and judge of things. 8
In this case, the patient didn’t seem to fully understand or appreciate (as seen by his lack of reaction during case-taking) the extent to which he suffered in his childhood due to the family’s financial troubles. Also, on the physical plane, he didn’t feel that he had any major symptoms due to hypertension, which again emphasises the lack of reaction.
Patient was advised to continue the anti-hypertensives.
REMEDY: Opium 200 three consecutive doses at hourly intervals (to take care of spillage and/or neglect)
200 (high) potency was chosen as there were many characteristic symptoms. 9
| DATE | FOLLOW UP | BLOOD PRESSURE | REMEDY GIVEN | REASON |
| 30/10/17 | First prescription | 140/80 mm of Hg | Opium 200 three consecutive doses at hourly intervals. Adequate rest. SL for one month | Based on repertorisation |
| 3/11/17 | Energy levels good. Headache episodes reduced. Had one episode of cold but it subsided on its own after 2-3 days. Generally better. | BP-130/84 mm of Hg | SL Adv : to reduce Telma 40 to Telma 20 and continue as OD dose. Continue Amlong2.5- 1 HS (patient’s physician informed ) | Remedy action still continuing Patient showing improvement.so no intervention required.10 |
| 3/12/17 | Overall better. Had one episode of mild Headache which reduced on its own | BP-130/84 mm of Hg | SL for two months | Remedy action still continuing Patient showing improvement.so no intervention required.10 |
| 4/2/18 | Overall better. Had no episodes of headache or recurrent coryza in the last two months | BP-126/84 mm of Hg | SL for two months Adv to stop Telma 20 and Amlog 2.5 | Remedy action still continuing Patient showing improvement.so no intervention required.10 |
| 4/4/18 | No episodes of headache or coryza in the last two months. Overall better | BP-120/84 mm of Hg | Adv to stop treatment |
Patient is under monitoring and continues to do well.
CONCLUSION
The above case demonstrates the potential role of individualised homoeopathic treatment for essential hypertension.
REFERENCES
- Oscar A. Carretero and Suzanne Oparil, Essential Hypertension, Originally published 25 Jan 2000 Circulation. 2000;101:329–335.Available from : https://doi.org/10.1161/01.CIR.101.3.329
- Matthew R Alexander, Meena S Madhur, David G Harrison, Albert W Dreisbach, Kamran Riaz , Hypertension, Feb 22, 2019 .Available from: https://emedicine.medscape.com/article/241381-overview#a3
- Tinsley R. Harrison, Harrisons Principles of Internal Medicine-Volume 2,16th Edition,United States of America,McGraw Hill,2005,page number1466
- Tinsley R. Harrison, Harrisons Principles of Internal Medicine-Volume 2,16th Edition,United States of America,McGraw Hill,2005,page number1468-1469
- https://www.icd10data.com/ICD10CM/Codes/I00-I99/I10-I16/I10-/I10
- Hompath Zomeo Software
- Boericke W,Pocket Manual of Homeopathic Materia Medica and Repertory-ninth edition,New Delhi, B Jain Publishers (P) Ltd.- page 486
- IACH – Prof. G. Vithoulkas, Opium by Kent. Available from: https://www.vithoulkas.com/learning-tools/materia-medica-kent/opium
- Roberts HA. The Principles and Art of Cure by Homoeopathy-Reprint edition, July 2014 India, IBPP, ,page number 121
- Close S. ‘The Genius of Homeopathy-Lectures and Essays on Homeopathic Philosophy’. Reprint edition, May 2014, New Delhi, IBPP, page number 192
ABOUT THE AUTHOR : Dr Sujata Naik, M.D (Hom.), a senior homoeopath, practising extensively in Mumbai for last 32 years across 3 centres with thousands of patients from India and abroad. She is the first International affiliate member of Faculty of Homoeopathy, UK.
She is also running a charitable OPD in Konkan region of rural Maharashtra at BKL Walawalkar Hospital, for the past 7 years with great success. With a team of passionate homoeopaths, Dr Naik has been involved in several research projects, including the one on homoeopathic management of chemotherapy induced peripheral neuropathy.
Dr Sujata received the best oral presentation award for her research study on “Homoeopathic treatment of resistant oral candiasis in patients with cancer” at 4th International Conference on Integrative Oncology held at Kochi, Kerala in February 2020.
Her talk on work regarding, “Homoeopathic treatment of chronic bronchial asthma in community setup” at LMHI 2019, Sorrento, Italy was highly revered.
The retrospective study on ‘Resistant Tinea’ carried out at the Rural Hospital was presented by Dr Sujata Naik at the LMHI 2018, Capetown and Faculty of Homoeopathy Congress 2018, Liverpool conferences and has been widely appreciated.
Dr Naik was awarded the 1st place for her Research Poster Presentation on PCOS and its homoeopathic management at the 1st International Conference on Alternative Medicine held by AYUSH (The Department of Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy) in November 2017 at Dubai.
Dr Sujata Naik is a prolific writer, columnist, orator. Dr Naik has been regularly invited as a speaker at various National and International Health Forums.
Her books “WELLNESS SHOTS” and “WELLNESS CAPSULES, a compilation of health and wellness tips posted on social media are hugely successful
CO-AUTHOR : Dr Runali Kelwalkar-Kore, M.D. (Hom.), Research Assistant at Dr Sujata Naik’s Homeopathy Clinic.