ABSTRACT-
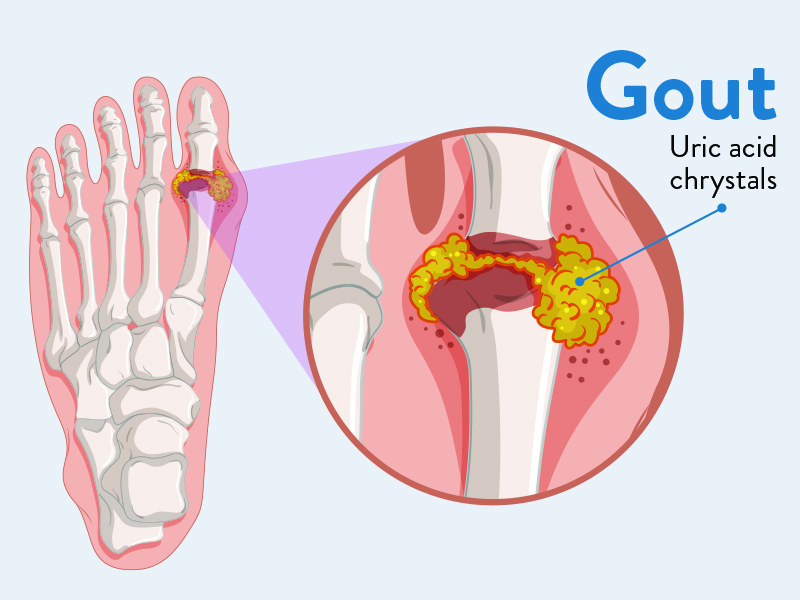
Gout is due to persistently elevated levels of uric acid in the blood .This occurs form a combination of diet ,other health problem and genetic factors. At high levels o uric acid crystals deposit in joints,tendons and surrounding tissues resulting and attack of gout. Gout occurs more commonly those who regularly drink beer or sugar sweetened, beverages or who eat foods that are high in purines. Diagnosis of gout may be confirmed by the presence of crystal in the joint fluid.
INTRODUCTION– Gout is caused by the deposition of monosodium urate monohydrate (MSUM) crystals at synovial joints. It has a prevalence of 1–2%, and is more common in men, in certain ethnic groups and with increasing age. Uric acid mainly comes from the metabolism of purines within the body but some is ingested with food. Gout is becoming more common with increased longevity and prevalence of metabolic syndrome
Causes of Hyperuricaemia and Gout –
•Diminished renal excretion (>90% of cases).
• Inherited reduction in renal tubular excretion of urate.
• Renal failure.
• Drug therapy (e.g. thiazide and loop diuretics, low-dose aspirin, ciclosporin).
• Lead toxicity (e.g. in ‘moonshine’ drinkers).
• Lactic acidosis (alcohol) Increased intake.
• Red meat, seafood, offal Over-production of uric acid.
• Myeloproliferative or lymphoproliferative disorders, chemotherapy for leukaemias, psoriasis.
• Increased de novo synthesis: cause unknown in most, rarely specific enzyme defects, e.g. glucose-6-phosphatase deficiency.
TYPES OF GOUT-
Acute gout: This presents with rapid onset of severe pain in a single distal joint, commonly the first metatarsophalangeal joint ,Other common sites include the ankle, midfoot, knee, hand, wrist and elbow. Examination reveals marked synovitis with swelling, red shiny skin and extreme tenderness. Periarticular swelling and fever may also be present. Symptoms are usually self limiting over 5–14 daysThe differential diagnosis includes septic arthritis, cellulitis and reactive arthritis.
Recurrent and chronic gout: Following an acute attack, many patients go on to experience a second attack within a year. The frequency of attacks increases with time. Involvement of several joints with continued MSUM deposition eventually leads to joint damage and chronic pain.
Chronic tophaceous gout: MSUM crystal deposits produce irregular firm nodules (‘tophi’) around extensor surfaces of fingers , forearms, elbows, Achilles tendons and ears. Tophi are usually a late feature of gout. Renal and urinary tract manifestations: Chronic hyperuricaemia may be complicated by renal stone formation (p. 190) and sometimes renal impairment due to interstitial nephritis caused by urate deposition in the kidney. This particularly affects patients with chronic tophaceous gout who are on diuretics.
Investigations–
• Joint aspiration reveals long, needle-shaped MSUM crystals, which are negatively birefringent under polarised light.
•Synovial fluid in acute gout appears turbid due to the high neutrophil count (>90%).
• Serum uric acid is usually elevated, but hyperuricaemia itself does not confirm gout
. • Equally, acute inflammation reduces levels, so a normal uric acid level does not exclude gout.
•Serum creatinine should be checked to exclude renal impairment.
•There is neutrophilia with a raised CRP in acute gout; FBC and ESR may detect myeloproliferative disorders during remission of the acute episode.
•Joint X-rays are usually normal in early gout. Changes of secondary OA and gouty erosions may develop with chronic disease. .
Predisposing factors should be addressed:
● Weight loss: advised in obese patients.
● Excess beer: avoid.
● Diuretics: stop if possible.
● High-purine diet (seafood, red meat and offal): avoid. Calcium pyrophosphate dihydrate crystal deposition Calcium pyrophosphate dihydrate (CPPD) crystal deposition within articular cartilage causes chondrocalcinosis.
Risk factors– include age, OA and primary hyperparathyroidism. Rarely, it is associated with metabolic disease (e.g. haemochromatosis, hypophosphataemia, hypomagnesaemia and Wilson’s disease). It is often clinically silent, but can cause episodes of acute synovitis (‘pseudogout’) or occur as a chronic arthritis that is associated with OA.
HOMOEOPATHIC MANAGEMENT OF GOUT-
1.BENZOIC ACID- Joint crack on motion.Tearing and stiches.Pain in tendoachillis,rheumatic gout very painful.Gout deposits.ganglion;swelling of the wrist.Pain and swelling in knees.Bunions of great toe.Tearing pain in the great toe.Highly colored and very offensive urine.
2.COLCHICUM AUTUMNALE- Inflammation of great toe,gout in the heel ,cannot bear to have it touched or moved. Tingling in the finger nails. Knee strike together,can hardly walk [knock knees].Edematous swelling and coldness of legs and feet.
3.URTICA URENS- Pain of acute gout ;deltoid; pain in ankles,wrist. Gout and uric acid diathesis.
4.ARNICA MONTANA- Gout.Great fear of being touched or approached.Pain in the back and limbs,as if bruised or beaten.Soreness after overexertion.deathly coldness of the forearm.
5.BRYONIA ALBA- Knees stiff and painful.Hot swelling of feet..Joints red, hot,swelling with stiches and tearing; worst on least movement.every spot is painful on pressure.constant motion of the left arm and leg.
6.LEDUM PALUSTRE- Gouty pain through the foot,limb and joints,but especially in the small joints .swollen,hot,pale.Gouty nodosities .Ball of great toe swollen.Ankle swollen.Soles painful.
References –
1] Davidson’s Essentials Of Medicine 2nd Edition 2016
2] BOERICKE’S NEW MANUAL OF HOMEOPATHIC MATERIA MEDICA WITH REPERTORY,37th Impression2016;B.JAIN PUBLISHER[P] LTD.
About Author
Dr. Balvant Thakur M.D Scholar [Homoeopathic Pharmacy] G.H.M.C Bhopal [MP]