
Authored by:
Dr Divya Vermaa, Dr Arun Kumarb
a( MD ( Practice of Medicine), Nehru Homoeopathic Medical College and Hospital, Delhi, India)
b(MD Scholar, Deptt of Practice Of Medicine, Bakson Homoeopathic Medical College, Greater Noida, Uttar Pradesh, India)
Abstract: Coronavirus is an acute viral illness caused by an RNA virus, SARS-CoV2. Presenting features may range from mild illness to pneumonia. Symptoms present as fever, cough, sore throat, and in severe cases difficulty in breathing and even death can occur. Early and accurate diagnosis is critical to reduce mortality and its spread. There are no vaccines or specific antiviral drugs available to prevent or treat corona virus infections except for symptomatic management of the case. Corona infection is a global threat to public health. This article provides a detailed overview on corona virus infection and how it affects humans at a cellular level with varied clinical manifestations. It also discusses its’ modes of transmission as its rapidity of transmission across countries threatens the health of millions, finally explaining the preventive measures that must be taken, and in brief, its’ conventional treatment and treatment available in homoeopathy.
Keywords: novel coronavirus, homoeopathy, genus epidemicus, dexamethasone
Abbreviations: RNA – riboxynucleic acid, SARS-CoV2 – severe acute respiratory syndrome coronavirus – 2, MERS – middle east respiratory syndrome, SARS – severe acute respiratory syndrome, ARDS – acute respiratory distress syndrome, COVID-19 – coronavirus infectious disease 2019, USA – United States of America, WHO – World Health Organization, ACE-2 – angiotensin converting enzyme 2, RBD – receptor binding domain, RDRP – RNA dependent RNA polymerase, IL – interleukin, TNF – tumour necrosis factor, PGE2 – prostaglandin 2, AST – aspartate transaminase, ALT – alanine aminotransferase, BUN – blood urea nitrogen, CRP – c-reactive protein, ESR – erythrocyte sedimentation rate, LDH – lactate dehydrogenase, RT-PCR – reverse transcriptase- polymerase chain reaction, DNA – deoxyribonucleic acid, Ig – immunoglobulin, POC – point of care, ICMR – Indian Council of Medical Research.
Introduction
Coronaviruses are enveloped, single stranded, positive strand RNA virusesbelonging to the family coronaviridae and the order nidovirales.[1] They are significant viral pathogens in humans and animals[2]. The word “corona” comes from a latin word for “crown”, it is named so for the crown like appearance of the virus under microscope. [3] There are four classifications of coronavirus – alpha, beta, gamma and delta. Human coronavirus are alpha and beta coronavirus which include seven forms of coronavirus that cause disease in humans. [4]
Epidemics of coronavirus developed because these viruses are transmitted from one species to another causing mutation in proteins that allow the virus to bind to cells and infect other cells more easily. [5] Human coronavirus mainly cause respiratory tract infection with spectrum of symptoms ranging from the common cold to pneumonia and ARDS. In humans we have noticed several coronavirus diseases in the past in which there has been transmission from one species to another leading to new outbreaks of coronavirus such as severe acute respiratory syndrome (SARS) [6][7] and middle east respiratory syndrome (MERS)[6]. The most recently discovered coronavirus causes coronavirus disease COVID-19.
COVID19 is caused by SARS-CoV2 (severe acute respiratory syndrome coronavirus 2) [6] also designated as 2019-nCoV that is 2019 novel coronavirus. This outbreak occurred in December 2019, which started in Wuhan City, Hubei province in China. [8] It has been shown through genetic analysis to be similar to bat coronavirus (96% related). [9] So it is suggested that this virus might have been transmitted from bats to humans. Huanan seafood market in Wuhan is the epicentre to this outbreak. This novel coronavirus shares approximately 80% sequence homology with SARS coronavirus. [10] Speculations have been rife about the virus being artificially created, however, evidence accumulated by mining the genomic data of the emergent virus has failed to substantiate such claims of a human-modified origin.[11] Reproductive ratio (R0) means how many persons can be infected by a carrier of COVID19 and ranges from 2.24 to 3.58. [12]
Scientists first identified a human coronavirus in 1960. Later that decade, researchers found a group of similar human and animal viruses and named them after their crown-like appearance. Alpha and Beta coronavirus affects humans. SARS-CoV2 popularly known as novel corona virus belongs to the Beta coronavirus lineage B group.[3]
Background
Scientists first identified a human coronavirus in 1960. Later that decade, researchers found a group of similar human and animal viruses and named them after their crown-like appearance. Alpha and Beta coronavirus affects humans.
- There are 2 alpha coronavirus that
cause illness in humans:
- First is HCov-229E discovered in mid 1960, more likely to infect immunocompromised patients and is less severe than others.
- Second is HCoV-NL63, this was discovered in 2003 in laboratory in Netherlands. It is the second most common coronavirus which affects humans.
- There are 3 lineages of beta coronavirus A, B, C.
- In lineage A
there are 2 viruses which cause infection in humans.
- First is HCoV-OC43 discovered in 1967 in laboratory in Maryland, USA. This is the most common stain of coronavirus to cause infection in humans. It causes the most severe presentation among HCoV strains (human coronavirus strains).
- Second is HCoV-HKU1, discovered in 2005 in a laboratory in Hong Kong. It is associated with febrile seizures. [3]
- In Lineage B
there are 2 viruses that cause infection in humans.
- First is SARS-CoV, SARS occurred in Guangdong province of China in 2002 and was transmitted from bats to civets and then to humans. This resulted in a worldwide outbreak which was recorded as early as february 2003 and lasted until july 2003. There were more than 8,000 total cases with 774 deaths with a fatality rate of 9.6%. A small outbreak in 2004 involved only four more cases. This coronavirus causes fever, cough, chill, myalgia, headache, and ARDS.[3][6][7]
- Second was SARS-CoV2 discovered in late 2019 in Wuhan, China, which has come to be known as novel coronavirus causing Coronavirus disease 2019 or COVID-19 causing the current worldwide pandemic with a mortality rate of 6.3%.[3]
- In lineage C there is MERS-CoV, causing MERS which occurred in 2012 and started in Saudi Arabia then quickly spread to several countries. It was reported that here the virus was transmitted from bats to camels then to humans. More than 2,400 cases have been recorded with 858 deaths and a fatality rate of 34.4%. This coronavirus is less contagious than SARS but more deadly. It can have fever, cough, dyspnoea, severe pneumonia and ARDS. [3][6]
Epidemiology
Wuhan is a city of 11 million people and is the seventh largest city in China. Hubei province is itself home to 50 million people. There were cases of pneumonia of unknowncause that occurred in december 2019 in this Hubei province of China. The first case was hospitalised on December 16, 2019. It is estimated that initial infections started as early as november 2019. After multiple sporadic cases began to increase throughout Hubei, China this virus was reported to WHO on December 31, 2019.
The first case of the COVID-19 pandemic in India was reported on 30 January 2020. The first death outside China was in The Philippines on february 2, 2020.Coronavirus disease was named COVID-19 by WHO on Feb 11, 2020. On March 11, 2020 COVID-19 was declared a global pandemic. On march 20, Italy surpassed China with the highest death toll. On april 2, the number of cases globally crossed 1 million. [13]
As of july 23, 2020, COVID-19 has been confirmed in over 15,501,959 individuals worldwide, has resulted in more than 632,638 deaths and 9,428,110 patients have recovered from this disease. More than 180 countries have reported confirmed cases of COVID-19 on all continents except Antarctica. [14]
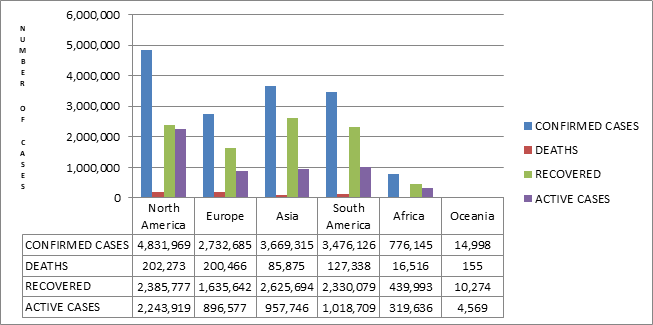
Figure 1: Data of COVID-19 in different continents as of 23 JULY, 2020. [14]
| Countries | Confirmed cases | Active cases | Recovered | Death |
| USA | 4,127,543 | 2,028,860 | 1,952,060 | 146,623 |
| BRAZIL | 2,242,394 | 627,220 | 1,532,138 | 83,036 |
| INDIA | 1,286,314 | 439,710 | 815,969 | 30,635 |
| RUSSIA | 795,038 | 201,816 | 580,330 | 12,892 |
| SOUTH AFRICA | 394,948 | 159,833 | 229,175 | 5,940 |
Table 1: Data of top 5 countries having cases of COVID19 as of 23 JULY, 2020[14]
*NOTE (ensure commas are in the correct positions for the above numbers)

Figure 2: Data of top 5 countries having cases of COVID-19 as of 23 JULY, 2020[14]
In a study conducted on severe acute respiratory illness (SARI) patients, the positivity of COVID-19 increased from 0 to 2.6 % in the 14th week. The median age of COVID-19 was 54 year and 83.3% were males, 81.4% were above 40 year of age. Positivity was higher in males (2.3%) and in 50-70 year of age group (4.4%). [15]
COVID-19 IN INDIA
The first case of the COVID-19 pandemic in India was reported on 30 January 2020. As of 23 July 2020, the number of confirmed cases is 1,286,314 confirmed cases, active cases 426,167, recoveries 782,606 and 29,861 deaths in the country. [16]
| STATE/UT | CONFIRMED CASES | ACTIVE | RECOVERED | DEATH |
| Maharashtra | 3,37,607 | 1,37,282 | 1,87,769 | 12,556 |
| Tamil nadu | 1,86,492 | 51,765 | 1,31,583 | 3,144 |
| Delhi | 1,26,323 | 14,954 | 1,07,650 | 3,719 |
| Karnataka | 75,833 | 47,075 | 27,239 | 1,519 |
| Andhra Pradesh | 55,588 | 31,763 | 32,127 | 823 |
Table 2: Data of top 5 state/union territory in India having maximum confirmed cases of COVID-19[16]
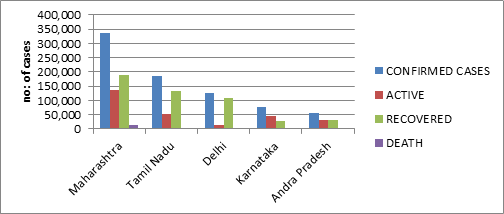
Figure 3: Data of top 5 state/union territory in India having maximum confirmed cases of COVID-19. [16]
42% of confirmed cases of coronavirus in India are between the ages of 21 and 40 years of age.
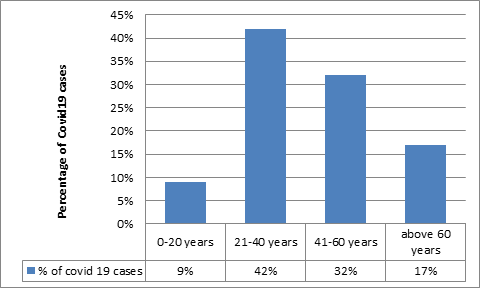
Figure 4: Age wise distribution of COVID-19 patients in India [17]
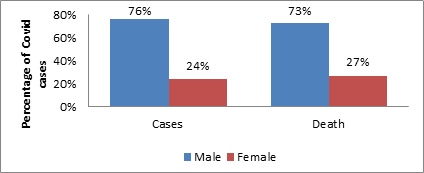
Figure 5: Gender distribution of COVID-19 cases and deaths in India as of April 7, 2020[18]
Structure of virus
Corona viruses have enveloped virions that measure approximately 120 nanometre in diameter having single stranded RNA. It has one of the largest RNA genomes known. It has club-shaped glycoprotein spikes on its surface, which appear like a crown under a microscope giving rise to its name corona which mean crown in Latin. The coronavirus genome encodes a spike protein (S), an envelope protein (E), a membrane protein (M), and a nucleoprotein (N). [3][19][20]
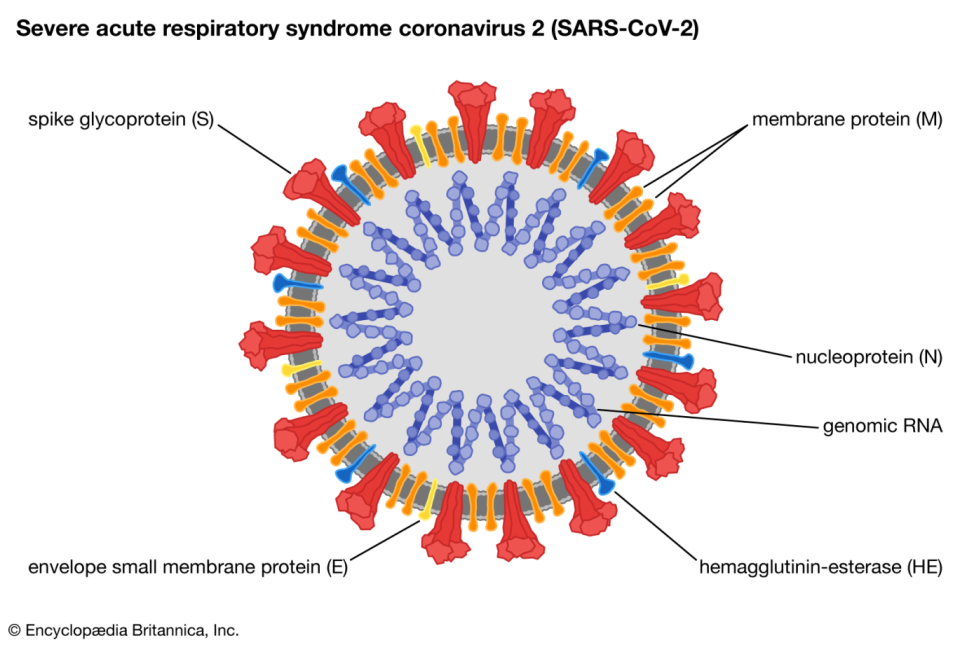
Figure 6: Structure of SARS-CoV2
Spike protein (S) is the most important surface membrane protein of corona virus. This protein is responsible for allowing the virus to attach to the membrane of its host cell. It contains a receptor binding domain which recognises a specific receptor, the ACE2 which is expressed in the lungs, heart, kidneys and intestine. This protein binds to ACE2 receptors. Spike proteins have 2 functional sub-units; S1 (binds to the host cell receptor) and S2 (mediates the fusion of viral and cellular membrane). Membrane protein (M) is most abundant on the viral surface and defines the shape of the viral envelope and acts as a central organiser for corona virus assembling and interacts with other structural proteins. Envelope protein (E) is the smallest of the major structural proteins. It is integral in assembly as well as releases the virus from the host cell and during viral replication it is largely localised to the site of intercellular trafficking, most specifically endoplasmic reticulum and the golgi apparatus.[3][19][21]
Underneath the surface protein we have the viral envelope. In contact with soap it will break down killing the virus. Underneath is capsid, and this is the protein shell which encloses the genetic material of the virus. Inside this capsid we have N protein, and this protein in bound to the virus’s single strand of RNA which is why all its genetic information is held to allow itself to replicate. The N protein appears to be multifunctional, and in particular, it essentially inhibits a lot of host cell defence mechanisms and assists the viral RNA in replicating itself and therefore creating new viral particles. [3][19]
Polybasic cleavage site that has not been previously observed in related lineage to B Betacoronaviruses and is a unique feature of SARS-CoV-2, was noted in the Indian SARSCoV-2. The mutation Arg408Ile in the spike protein of one of the Indian sequences is noted to be in the RBD and Ala930Val is located in the S2 domain. However, both are away from the ACE2 receptor-binding interface. Mutations in the spike protein sequences of SARS-CoV-2 observed currently are localised over the S1 and S2 domains. [22]
Pathogenesis
The virus is spread through droplet infection and travels to the nasal or oral cavity and gets in contact with mucus membrane. Initially it gets into the upper airways of the nasal and throat area that give rise to symptoms like stuffy nose, fever, sore throat, etc. It is within the mucosal epithelium of the upper respiratory tract where primary viral replication occurs. Then it gets further down into the respiratory system and into the lung epithelial cells where further viral replication occurs. [3][19][23]
The SARS-COV2 binds by S protein to the ACE2 receptor on type two pneumocytes. The host cells have proteases which are enzymes that break down protein and these cleave spike protein. This process activates the protein in order to trigger the process of membrane fusion before injecting the viral genome into the host cell which is direct cell entry. It releases the single stranded RNA into actual cytoplasm of type two pneumocyte. The virus may also enter the cell via endocytosis, once inside the cell, virus specific RNA and protein are synthesised within the cytoplasm. [3][19[23][24]
The virus can use the host cell ribosome and convert mRNA into protein called translation. It can also use another enzyme called RNA dependent RNA polymerase (RDRP). It takes single stranded RNA and synthesises into more RNA. The protein formed from translation is now proteolytically cleaved by proteases to form a different viral component that is a nuclear capsid, enzymes and spike proteins. This viral component gets incorporated with single stranded RNA and bud off from type two pneumocytes forming tons of viral particles. In this process type two pneumocytes are destroyed and various inflammatory mediators are released which stimulates the macrophage which start to secrete specific cytokines like IL-1, IL-6, TNF-ἀ.[25][26][27]These cytokines enter the blood stream and cause endothelial cells to undergo vasodilation and increase the capillary permeability leading to accumulation of fluid in interstitial space compressing alveoli. Some of the fluid also enters into the alveoli causing alveolar oedema and an increase surface tension leading to alveolar collapse. The alveolar walls become inflamed and thickened and fill the alveolus with fluids which can impair the gas exchange and lead to hypoxaemia and shortness of breath further leading to acute respiratory distress syndrome or ARDS. [3][19][20][23][24][28]
All these inflammatory mediators attract neutrophils inside the alveolus which release reactive oxygen species that is proteases to destroy virus, which damages type one and two pneumocytes too, finally leading to consolidation inside the alveolus. It alters the gas exchange leading to hypoxaemia. TNF-ἀ, IL-1 and IL-6 when in high concentration can travel to the hypothalamus and hypothalamus releasing specific prostaglandins like PGE2 and increases the body temperature leading to fever. [3][19] [23][24]
This cascade of inflammatory mediators causes an uncontrolled systemic inflammatory response syndrome. It increases capillary permeability within systemic circulation, fluid leaks out leading to a decrease in overall blood volume. Vasodilation causes decreased peripheral resistance too. Following these events the blood pressure falls causing hypotension, decreasing perfusion to different organs and leads to multiple organ failure. Kidney can be affected leading to increased levels of BUN, creatinine. Liver may also get damage and start to release AST, ALT, bilirubin and acute phase reactive proteins like CRP, fibrinogen, IL-6.[3][23]
Transmission
- Human to human transmission is the primary means of transmission for covid19. It occurs through respiratory droplets that are exposure to sneezing and coughing, very similar to the spread of other respiratory viruses. It could be transmitted airborne at least within the vicinity of the respiratory droplets. It requires close contact with infected individual that is within six feet or 2 metres as droplets typically do not travel beyond this range. SARS-CoV-2 has been detected in faeces in patients in Washington, US, but its role in transmission is uncertain. Other coronavirus have been shown to cause gastro intestinal infections like SARS caused diarrhoea in approximately 10 to 20 % of patients and could spread through faeces.[29] Coranavirus RNA in blood has also been reported in some but not all studies that have tested for it. However, the likelihood of blood borne transmission appears low; respiratory viruses are generally not transmitted through the blood borne route. SARS-CoV-2 can be transmitted before the development of symptoms and throughout the course of illness, particularly early in the course. Transmission of SARS-CoV-2 from asymptomatic individuals (or individuals within the incubation period) has also been seen. Asymptomatic patients are still able to transmit infection. This raises concerns for the effectiveness of isolation. [24][28]
- Fomites: The virus can be transmitted through indirect objects like fomites. Respiratory droplets can land on some objects which becomes contaminated with the virus and when any individual touches that object and then touches their nose, eyes or face then they may have a transmission through that mechanism.
- Animal contact: SARS-CoV-2 came from animal species to humans, but the ongoing risk of transmission through animal contact is uncertain. There is no evidence suggesting animals (including domesticated animals) are a major source of infection in humans.[28]
Clinical Presentation
The incubation period for COVID-19, which is the time between exposure to the virus (becoming infected) and symptom onset, is on average 5-6 days, however can be up to 14 days. During this period, also known as the “presymptomatic” period, some infected persons can be contagious [30]. A patient can be asymptomatic or have mild to severe illness or can also lead to death. Most common symptom of COVID-19 is fever [29]which is almost always present. Second most common symptom is cough [29] which may be non-productive or productive but mostly it is a dry cough. Next we have shortness of breath, difficulty in breathing, malaise and fatigue. Other symptoms that are less common include myalgia, headache, confusion, rhinorrhoea, conjunctivitis, and sore throat. Gastrointestinal symptoms like diarrhoea, nausea and vomiting can also be seen which is extremely rare. [25][31][32]
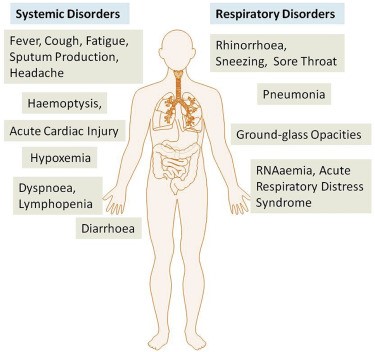
Figure 7: The systemic and respiratory disorders caused by COVID-19 infection.
Approximately 20% of cases have a critical presentation which may include pneumonia, renal failure, ARDS and death due to multiple organ failure. This severe illness seems to occur in older individuals and those with underlying co-morbidities which include cardiovascular disease, diabetes mellitus, hypertension, chronic lung disease, cancer, chronic kidney disease, obesity, smoking, etc.[25] Most people (about 80%) recover from the disease without requiring hospital treatment.
Laboratory findings
Indicate neutrophilia, lymphopaenia, increased AST, ALT and bilirubin, increase creatinine and increase BUN. General markers of inflammation are elevated like CRP, ESR, IL-6, LDH, D-dimer, ferritin which can lead to high mortality rates. [26][33]
Diagnosis
Diagnosis is done by viral genome detection by RT-PCR (reverse transcriptase- polymerase chain reaction).The test detects the presence of viral RNA in human samples. RT-PCR is highly specific (i.e. 95-97%) but has a low sensitivity of 60-70%. [34]
To perform RT-PCR some of the extraction from a nasopharyngeal swab is added to a solution containing reverse transcriptase, nucleotide and primers that are complementary to specific SARS-CoV2 target sequence. If the viral RNA is present the primer attaches to the RNA strand and then reverse transcriptase synthesises a cDNA strand. Once we got cDNA denaturation, annealing and extension are performed. First step is denaturation that is heating up of these ingredients to 96 degree celsius, this break opens all the bonds between two strands of cDNA followed by second step that is annealing which requires primers. During this step, one cools down everything to 55 degree Celsius and this allows primers to bind to their complementary sequences. Then it is followed by third step extension in which we heat back to 72 degree celsius and taq polymerase latches on to the primers which grab some free nucleotides and assembles a new DNA strand. After several steps if there was SARS-CoV2 RNA in the original samples, you have amplified DNA from that sample that can be detected. [35]
Rapid diagnostic test (RDT): This is a qualitative (positive or negative) lateral flow assay that is small, portable and can be used at point of care (POC). They detect patient’s antibodies (IgM and IgG) or viral antigen. [36]
Chest X Ray of coronavirus patient show consolidation with bilateral pulmonary infiltrates.
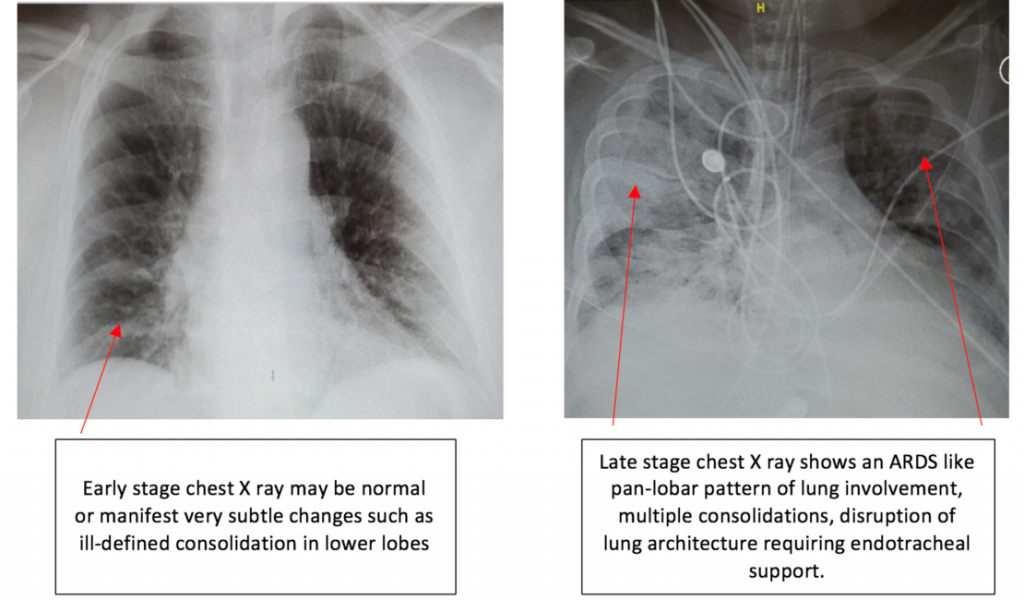
Figure 8: Early and Late stage X-Ray findings of Covid-19 patient [37]
CT Scan shows ground glass opacities which are bilateral as well as multilobar consolidation.[7][38]
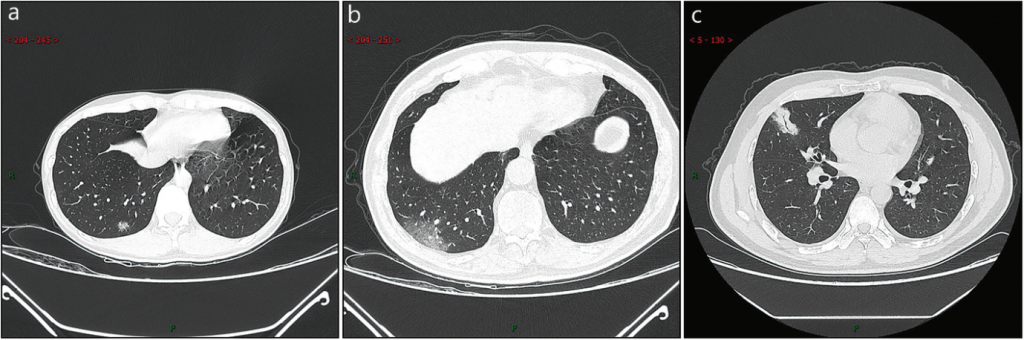
Figure 9: CT imaging of ultra-early stage. A A 33 years old female with patchy ground-glass opacities after occupational exposure. B A 67 years old male with a history of contact with infected patients, showing large ground-glass opacity. C A 35 years old female exhibiting large consolidated opacity with air-bronchogram inside after occupational exposure. [39]
Prevention
Preventive measures can only limit the spread of cases. Preventive strategies are focused on the isolation of patients and careful infection control. If a person is coming from area where there is viral outbreak then Quarantine for 14 days is suggested.
Following are general recommendations: [40][41][42]
- Wash your hands frequently with soap and water for 20 seconds or use an alcohol based sanitizer.
- Avoid close contact within 2 meters with sick patients.
- Respiratory hygiene – avoid touching mouth, nose, eyes, face if hands are not washed.
- Face mask such as N95 or FFP3 masks should be used to prevent transmission of the pathogen.
- People with symptoms of acute airway infection should keep their distance, cover coughs or sneezes with disposable tissues or clothes and wash hands.
- Individuals that are immunocompromised should avoid public gatherings.
- Avoid travel to affected areas.
- Avoid going to school or workplace if you are sick as it may spread the virus to others.
- Considering the reports of a high number of infected healthcare workers, measures should be taken to build bio security wards and they should be provided personal protective equipment.
Conventional Treatment
There is no specific drug and vaccine currently available for COVID19 infection. So supportive care is provided like hydrating the patient and treating any co-infections. Many patients don’t even require hospitalization; they can recover at home. The treatment followed is purely symptomatic based on the presenting symptoms of the patients. As per WHO treatment of acute co-infections, for suspected or confirmed mild COVID-19 cases, the use of antibiotic therapy or prophylaxis should not be used. For suspected or confirmed moderate COVID-19 cases, antibiotics should not be prescribed unless there is clinical suspicion of a bacterial infection. Prevention of complications in patients (adults and adolescents) hospitalized with COVID-19, pharmacological prophylaxis should be used, such as low molecular weight heparin (e.g. enoxaparin), according to local and international standards, to prevent venous thromboembolism, when not contraindicated. For those with contraindications, use mechanical prophylaxis (intermittent pneumatic compression devices). WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia. [43] WHO welcomes preliminary results about dexamethasone use in treating critically ill COVID-19 patients.[44]
Treatment and prevention available in Homoeopathy
Homoeopathy is a science based on symptomatic treatment of the patient. It is a holistic treatment which treats the patient instead of the disease: that is cure effected by the removal of the whole of the perceptible signs and symptoms of the disease which occur due to internal alteration of the vital force. In case of an epidemic the totality of symptoms of the epidemic is noted by writing down the characteristic symptoms of several cases of this kind including more of the peculiarities of this collective disease as each single epidemic is of a peculiar, uniform character common to all individuals attacked and when this character is found in the totality of symptoms common to all, it guides us to the discovery of a homoeopathic remedy suitable for all the cases which is called as genus epidemicus. [45]
The Central Council for research in Homoeopathy (CCRH) under the Ayush Ministry, India recommended that the homoeopathic medicine Arsenicum Album 30 could be taken on an empty stomach for three days as a prophylactic against coronavirus infection. The dose should be repeated after one month by following the same schedule in case the COVID19 infection prevails in the community. Various other medicines found to be effective in symptomatic management of the coronavirus cases are Arsenicum album, Bryonia alba, Rhus toxicodendron, Belladonna, Gelsemium, Eupatorium perfoliatum etc, which should only be taken under expert guidance as they are prescribed on the basis of symptoms similarity.[46]
Dr. Aditya Kasariyans from Iran in collaboration with Dr Rajan Sankaran (Head of “The Other Song”- International Academy of Advanced Homoeopathy in Bombay, India) collected symptoms from 40 cases of COVID-19 in Iran. From the detailed study of these symptoms he short listed Arsenicum album, Camphor, Carbo vegetabilis and Veratrum album. With reference to the genius of the disease, its individuality; sudden collapse, cold sweat and a relative absence of restlessness, he suggested Camphor as the genus epidemicus and to use it as a treatment (1M in water every 3 hours) and prophylactic (1M in pills twice a day for 2 days). Camphor 1M was given in cases and significant improvement was seen. [47]
According to WHO and ICMR, the disease advance has been divided in following stages and Dr. Prafull Vijayakar (Founder and Director of Predictive Homoeopathy) recommended homoeopathic treatment in each stage:
Stage 1: Sporadic stage where patient presents with mild symptoms generally recovers on its own.
Stage 2: Cluster stage that is corona positive cases but asymptomatic patients where the disease is in hiding stage, homoeopathic treatment advised is spraying Sepia 200 in the area of containment or with one dose of Sepia 200 internally.
Stage 3: Community spread is fast spread with high fever, cough, aches, loose motion, difficulty breathing and weakness. For mild cases Sepia 200 is recommended, but if there is breathing difficulty or pneumonia like symptoms he recommended Veratrum album 50M.
Stage 4: Epidemic, which have severe symptoms like pneumonia, respiratory distress, inflammation of blood vessels and can lead to sudden death. In this stage he recommended Veratrum album 50M, Lachesis mutus 200 or Crotalus horridus 200 based on the disease picture present. [48]
Conclusion
COVID-19 has evolved as a global life-threatening public health concern, affecting more than 15 million individuals in more than 180 countries. The physician should be aware about the varied clinical manifestations of this condition and ensure an early and adequate treatment plan. Future directions to combat this dreadful disease aim at methods of social distancing, staying indoors, use of masks, avoiding social gatherings and avoiding contact with infected persons. Many countries are following lockdown which showed reduced intensity of COVID-19 spread, as prevention is the only measure today which can save the world from COVID-19. Following all the preventive measures can bring R0 below 1 which means each existing infection causes less than one new infection and the disease will decline and eventually die out. Provisions should be taken to provide quarantine centres, as many as possible isolation beds in hospitals and COVID care centres according to the severity of illness as patients who are asymptomatic or having mild symptoms can be managed at home. Development of vaccine and antiviral drug regimen should also be focused upon. Investment should be made on serological assays to detect the antibodies IgG and IgM in blood, to test for the infection. Antibody-based test can help identify individuals who got cleared of the viral infection but were once infected. Antibody tests with similar accuracy and specificity as the RT-PCR test are needed for mass screening.
This panic state is also causing psychological changes in people which lower their immunity. Homoeopathy has a great scope in management of cases of COVID-19 as it considers the physical as well as mental state of the patient and its symptomatic prescription boosts the immunity which helps our immune system itself to annihilate the virus from our body. Homoeopathy has more than a thousand proven drugs which guide the physician to an accurate prescription according to the severity of disease and individual picture of the patient. So apart from conventional treatment, homoeopathic management should also be focused in order to lessen the burden of morbidity worldwide.
Few homoeopathic drugs which can be effective in COVID-19[49,50]
- Aconitum napellus: A state of fear, anxiety; anguish of mind and body. Physical and mental restlessness, fright. Acute, sudden, and violent invasion, with fever, call for it. Sudden sinking of strength. Serous membranes and muscular tissues affected. Burning in internal parts. Influenza. Causes only functional disturbance, no tissue changes and shows no periodicity. Influenza. Delirium is characterised by unhappiness worry, fear, raving, rarely unconsciousness. Oppressed breathing on least motion. Cough, dry, short, hacking; worse at night and after midnight. Loud, labored breathing. Child grasps at throat every time he coughs. Shortness of breath. Coldness and heat alternate. Thirsty. Chilly if uncovered or touched. Dry heat, red face. Coldness and heat alternate.
- Bryonia alba: Mucous membranes are all dry. Listless, irritable people lying or motionless. Vertigo from raising the head, pressive headache; dry, parched lips, mouth; bitter taste, sensitive epigastrium, and feeling of a stone in the stomach; stools large, dry, hard. Dry mouth- thirstless; or thirst for large quantities at large intervals. Complaints apt to develop slowly. Aching of muscles. The general character of the pain stitching, tearing. Hacking cough from irritation in upper trachea. Cough, dry, at night; must sit up; worse in a warm room, after eating or drinking, with vomiting, with stitches in chest, and expectoration of rust-colored sputa. Frequent desire to take a long breath. Pulse full, hard, tense, and quick. Chill with external coldness. Internal heat. Dull but not sleepy. Bodyache > pressure < movements. Business thoughts. Ailments from anger, mortification.
- Gelsemium sempervirens: General prostration. Dizziness, drowsiness, dullness, and trembling. Slow pulse, tired feeling, mental apathy. Desire to be quiet, to be left alone. Apathy regarding his illness. Absolute lack of fear. Delirious on falling to sleep. Heaviness above eyes and of upper eyelids with occasional heaviness of limbs. Sleepy but cannot sleep. Timid and apprehensive. Ailments from vexation emotional excitement, fright & fear. Acute coryza, with dull headache and fever. Dry cough, with sore chest. Aphonia; acute bronchitis, respiration quickened, spasmodic affections of lungs and diaphragm. Wants to be held, because he shakes so. Pulse slow, full, soft, compressible. Chilliness up and down back. Heat and sweat stages, long and exhausting, thirstless, prostrated. Chill, without thirst, along spine; wave-like, extending upward from sacrum to occiput.
- Antimonium tartaricum: Rattling of mucus with little expectoration has been a guiding symptom. There is much drowsiness, debility and sweat characteristic of the drug. Great despondency. Fear of being alone. Muttering, delirium, and stupor. Coated, pasty, thick white, with red edges. Dizziness, with cough. Dyspnoea relieved by eructation. Cough and dyspnoea better lying on right side. Rapid, short, difficult breathing; seems as if he would suffocate; must sit up. Oedema and impending paralysis of lungs. Intense heat. Copious perspiration. Cold, clammy sweat, with great faintness. Intermittent fever with lethargic condition. Excessive weakness. Excessive sleep. Irritability. Thirstless or sips of water often. Aversion to milk.
- Pulsatilla nigricans: Dry mouth yet thirstless or changeable thirst. Mild, meek, weeping, wants mother near, carrying, caring, consoling. Wants doors and windows open. Changeable: thermals, thirst, etc. Involuntary moaning with fever. Loss of smell. Alternations of taste and loss of taste. Dry cough in evening and at night; must sit up in bed to get relief; and loose cough in the morning. Short breath, anxiety, and palpitation when lying on left side. Smothering sensation on lying down. Chilliness, even in warm room, without thirst. Chill about 4 pm. Intolerable burning heat at night. One-sided sweat; pains during sweat. External heat is intolerable, veins are distended. During apyrexia, headache, diarrhoea, loss of appetite, nausea.
- Arsenicum album: Desire sips of water. Desires warm food and drinks. Fastidious. Anxiety about health. Graceful. Midnight aggravation. Chilly feeling. Debility, exhaustion, and restlessness, with nightly aggravation, are most important. Great exhaustion after the slightest exertion. Burning pains. Unquenchable thirst. Burning relieved by heat. Changes place continually. Fears, of death, of being left alone. Thinks it useless to take medicine. Cannot bear the sight or smell of food. Great thirst; drinks much, but little at a time. Unable to lie down; fears suffocation. Air-passages constricted. Cough worse after midnight; worse lying on back. Wheezing respiration. High temperature. Periodicity marked with adynamia. Septic fevers. Intermittent. Delirium; worse after midnight. Great restlessness. Great heat about 3 a.m.
References
- S. Su, G. Wong, W. Shi, et al. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses, Trends in Microbiology, 2016 Jun;24(6):490-502.
- Richmann DD, Whitley RJ, Hayden FG, Clinical virology, 4th edition. Washington: ASM press, 2016.
- Weiss SR, Navas- Martin S. Coronavirus Pathogenesis and the Emerging Pathogen Severe Acute Respiratory Syndrome Coronavirus, Microbiology and molecular Biology rev. 2005 Dec; 69(4): 635-664.
- S. PerlmanJ. Netland. Coronaviruses post-SARS: update on replication and pathogenesis, Nat Rev Microbiol, 2009 Jun; 7(6):439-50.
- Patrick C. Y. Woo, Susanna K. P. Lau, Carol S. F. Lam,Candy C. Y. Lau, Alan K. L. Tsang, John H. N. Lau,et al. Discovery of Seven Novel Mammalian and Avian Coronaviruses in the Genus Deltacoronavirus Supports Bat Coronaviruses as the Gene Source of Alphacoronavirus and Betacoronavirus and Avian Coronaviruses as the Gene Source of Gammacoronavirus and Deltacoronavirus, J Virol. 2012; 86(7): 3995–4008.
- Lin L, Lu L, Cao W,Li T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection- a review of immune changes in patients with viral pneumonia, Emerg Microbes Infect. 2020 Dec; 9(1): 727-732.
- Zhong N, Zheng B, Li Y, et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003,Lancet. 2003; 362(9393):1353-8.
- A. Du Toit , Outbreak of a Novel Coronavirus, Nat Rev Microbiol. 2020;18(3):123.
- KG. Andersen, A. Rambaut, W. Ian Lipkin, EC. Holmes, Robert F. Garry . The proximal origin of SARS-CoV-2. Nature Medicine. 2020; 26, 450–452.
- J Zheng. SARS-CoV-2: an Emerging Coronavirus that Causes a Global Threat. Int J Biol Sci. 2020; 16(10): 1678–1685.
- Pranab Chatterjee, Nazia Nagi, Anup Agarwal, et al. The 2019 novel coronavirus disease (COVID-19) pandemic: A review of the current evidence. Indian J Med Res, 2020; 151:147-159.
- Zhao S, Lin Q, Ran J, Musa SS, Yang G, Wang W, et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int J Infect Dis, 2020;92 : 214-7.
- World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report jan- may, Geneva: WHO; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
- Worldometer. Coronavirus Update (Live) – Worldometer. Available from: https://www.worldometers.info/coronavirus/
- Nivedita Gupta, Ira Praharaj, Tarun Bhatnagar, et al. Severe acute respiratory illness surveillance for coronavirus disease 2019, India, 2020. Indian J Med Res, 2020; 151:236-240.
- Government of India. Coronavirus disease 2019 (COVID-19). Available from: https://www.mygov.in/covid-19/
- Press Information Bureau, Government of India. Advisory for Corona virus. Available from: https://pib.gov.in/PressReleseDetailm.aspx?PRID=1611125
- Times of India. Available from: https://timesofindia.indiatimes.com/india/63-of-covid-19-deaths-in-indian-among-60-plus/articleshow/75018702.cms.
- Walls AC, Park Y, Tortorici MA, Wall A, et al. Structure, Function and antigenicity of the SARS-COV-2 Spike Glycoprotein. Cell, 2020; 181(2): 281-292.
- Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, Epidemiology, Pathogenesis and control of COVID-19. Viruses, 2020; 12(4): 372.
- Schoeman D, Field BC. Coronavirus envelop protein: current knowledge. Virol J. 2019;16
- Pragya D. Yadav, Varsha A. Potdar, Manohar Lal Choudhary, et al. Full-genome sequences of the first two SARS-CoV-2 viruses from India. Indian J Med Res, 2020; 151:200-209.
- Li X, Geng M, Peng Y, Meng L, Lu S. Molecular immune pathogenesis and diagnosis of COVID-19. J Pharm Anal 2020;10(2):102-108.
- Rabi FA, Al ,ZOUBI MS, Kasasbeh GA, Salameh DM, Al Nasser AD. SARS-CoV-2 and Coronavirus Disease 2019: What we know so far, Pathogens. 2020; 9(3): 231.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 2020; 395.
- Rohtang HA, Byrareddy ON. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak, Journal of Autoimmunity- Elsevier. 2020; vol 109.
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus–induced lung injury. Nat. Med. 2005; vol 11: 875–879.
- Guo Y-R, Cao Q-D, Hong Z-S, Tan Y-Y, Chen S-D, Jin H-J, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Mil Med Res. 2020; 7 (1):11.
- Guan WJ, Ni ZY, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708‐1720.
- Bhatnagar T, Murhekar MV, Soneja M, et al. Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use. Indian J Med Res. 2020;151(2 & 3):184‐189.
- Ren LL, Wang YM, Wu ZQ, et al. Identification of a novel coronavirus causing severe pneumonia in human: a descriptive study. Chin Med J (Engl). 2020; 133(9):1015‐1024.
- Carlos WG, Dela Cruz CS, Cao B, Pasnick S, Jamil S. Novel Wuhan (2019-nCoV) Coronavirus. Am J Respir Crit Care Med. 2020; 201(4):P7‐P8.
- Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA. 2020; 323(11):1061–1069.
- Mossa-Basha M, Meltzer CC, Kim DC, Tuite MJ, Kolli KP, Tan BS. Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Panel [published online ahead of print, 2020 Mar 16]. Radiology. 2020;200988.
- Coffin JM, Hughes SH, Varmus HE, Retrovirus, Cold Spring Harbor Laboratory Press, 1997.
- Kobokovich A, West R, Gronvall G. “Global Progress on Covid-19 Serology Based Testing”. Johns Hopkins Center for health Security.
- Fatima S, Ratnani I, Husain M, et al. (April 12, 2020) Radiological Findings in Patients with COVID-19. Cureus 12(4): e7651.
- J. Lei, J. Li, X. Li, X. Qi. CT imaging of the 2019 novel coronavirus (2019-nCoV) pneumonia Radiology, 2020; 295(1).
- Jin, Y., Cai, L., Cheng, Z. et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Military Med Res 7, 4 (2020).
- World Health Organization. Coronavirus disease 2019 (COVID-19). Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public.
- Centre of disease control and prevention. Coronavirus disease 2019 (COVID-19). Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html.
- Sandip Mandal , Tarun Bhatnagar , Nimalan Arinaminpathy, et al. Prudent public health intervention strategies to control the coronavirus disease 2019 transmission in India: A mathematical model-based approach. Indian J Med. 2020;151: 190-199.
- Frieman M, Baric R. Mechanisms of severe acute respiratory syndrome pathogenesis and innate immunomodulation. Microbiol Mol Biol Rev. 2008 Dec; 7(4): 672-85.
- World Health Organisation: www.who.int/news-room/detail/16-06-2020-who-welcomes-preliminary-results-about-dexamethasone-use-in-treating-critically-ill-covid-19-patients.
- Hahnemann S; Organon of medicine, 5and 6th edition; Dudgeon RE and Boericke W (translator); Modern Homoeopathic Publication, Kolkata, 2006.
- Press Information Bureau, Government of India. Advisory for Corona virus. Available from: https://pib.gov.in/pressreleasepage.aspx?prid=1600895
- https://facultyofhomeopathy.org/members-area/covid-19/homeopathy-for-coronavirus-covid-19-infection-dr-aditya-kasariyans-and-dr-rajan-sankaran/
- Dr Prafull Vijayakar, Predictive Homoeopathy Official. April, 2020. Available from: https://youtu.be/Bp9fXD6gugl
- Boericke W, Boericke’s New Mannual of Homoeopathic Materia Medica with Repertory, India. B.Jain publisher; 2007
- Clarke J H, A Dictionary of Practical Materia Medica, London, The Homoeopathic Publishing Company; 1902.



