Why should we do what kind of research in medicine, and especially in homoeopathy? Proving that a medicine or a method works better than placebo may be required by insurance companies and politicians, but patients benefit more from improving diagnosis and treatment. Diagnosis and treatment are interlinked, without a proper diagnosis there might be no optimal treatment. The basic questions of the patient coming to a doctor are “What’s wrong with me?” and “Will this medicine/treatment work for me?” This should be reflected in research and the results must be relevant for daily practice. Proving hypotheses is still regarded as the core task of (medical) science, but requires highly specialised professionals. This is for doctors mainly concerned with treating patients. Their scientific task is to critically reflect their knowledge and preconceived ideas to improve what they are doing. Their questions do not concern the overall efficacy of a medicine or method, but the reproducibility of each consideration made in daily practice. Such a consideration might be: “This patient has an aversion to salt food, what does that mean in terms of preferred medicines?” According to the information in Kent’s repertory, based on provings and experience in the past, this symptom indicates the medicine Graphites, but also Natrium muriaticum. Is this true, because the opposite symptom ‘Desire for salt food’ is more well known for Natrium muriaticum? How much more likely will a curative effect of Graphites or Natrium muriaticum be if the patient has this symptom? We show how much these repertory-entries could have been influenced by chance and/or bias. Hitherto there has been hardly any scientific and statistical evaluation of our repertory-entries, despite the fact that these are so vital for our success.
What’s wrong with me?
How do we diagnose an illness, e.g. pneumonia? This is a step-by-step process, where several consecutive symptoms increase our suspicion that the patient has pneumonia. Then we do some targeted investigations to confirm this diagnosis.
Suppose you speak to a patient on the telephone and he tells you that he has a fever. As such, still, nothing to worry about, this is most frequently a harmless viral infection.
However, then he tells you that he has a cough and dyspnoea and you can hear that his breathing is accelerated. At that moment you know that the infection is probably in the airways and impairing oxygen transfer. This could be serious.
So, you invite the patient at your office. He comes in and you notice that he holds his chest while coughing. From this, you conclude two things: he coughs when entering a warm room from the cold outside and the cough is painful.
Then you listen to his lungs and measure C-reactive protein (CRP) in his blood.
You hear signs corresponding with pneumonia and the CRP is positive. You can even tell that you estimate the probability that he has pneumonia is about 80%. Now you may opt for an X-ray to be even more certain or start treating.
What happened here? You used the knowledge you were taught in medical training, and possibly also your own experience. Doctors before you (maybe also you) noticed that patients with these symptoms are more likely to have pneumonia than a common cold. There is one extra symptom, the fact that the patient coughs when he enters a warm room from the cold, that you don’t need for your diagnosis, but can be helpful when selecting a homoeopathic medicine.
Will this medicine work for me?
Now the diagnosis is quite certain, you prescribe medicine(s) for his infection and cough. Then the patient asks “Will this medicine work for me?” and your answer is “Of course, there is scientific proof that this medicine works.” However, the patient is not convinced, because he used this medicine before and then it didn’t work. He asks again “What is the chance that this medicine works for me?”
Can you answer this question? Suppose you want to prescribe Zinc acetate to alleviate the symptoms. Retrieve the meta-analysis of this medicine by Hemilä and Chalker (http://www. biomedcentral.com/1471-2296/16/24 ), this paper is free of charge and you have the highest level of evidence. The paper says that this medicine reduces the sore throat by 18%, the cough by 46% and shortens the duration of muscle ache by 54%. However, this is compared to placebo and it is unlikely that you considered giving a placebo, so these figures are not representative for daily practice. The paper doesn’t mention the chance that the medicine will work and certainly not in which patient it will work. The 46% reduction of cough does not mean that the cough is reduced in 46% of the patients, but that the average patient (that doesn’t exist) has 46% reduction of cough compared to placebo. This problem exists for most conventional medicines: you know it works better than placebo (if there is proof at all), but not in which patient it works.
Something is strange here: you can tell the patient the probability of pneumonia, but not the probability of effective medicine. Furthermore, notice that the knowledge you have about diagnosis is different from your knowledge about the medicine you prescribe. The knowledge about diagnosis comes from daily practice and can be used in daily practice, the knowledge about the medicine comes from an experimental test and you don’t know what it means in daily practice. The outcome of a randomised controlled trial (RCT) is also not valid for patients with other complaints than the tested condition because these patients (with co-morbidity) are excluded from participating in RCT.
Now we will show that this is different in homoeopathy and how we can translate daily experience into research.
Proving or improving
Above we showed that a proven medicine is not necessarily effective in the individual patient; proof by RCT means that it is quite certain that the medicine has an effect beyond placebo. This is about hypothesis testing: the hypothesis is that the medicine does not work better than placebo, then the medicine is compared with placebo in an experimental situation. The statistical analysis of the outcome of this test is a yes-or-no answer: the medicine works better than a placebo or not.
There is this joke about frequentist statistics: “What does a statistician call it when the heads of 10 rats are cut off and 1 survives?”. Answer: “Nonsignificant.”
The yes-or-no statistics applied in proving a medicine is classical (also called frequentist) statistics, testing a specific hypothesis. However, there is another statistical method that does not test a hypothesis but estimates the chance that something will happen given a specific symptom or condition. The chance that a patient has pneumonia increases if the patient has rapid breathing. This statistical method is called Bayesian statistics. This method will be explained more extensively throughout this book.
Bayesian statistics are generally not used to proof hypotheses but can be very useful in improving daily practice.
Now a joke about a Bayesian statistician: “A Bayesian: one who asks you what you think before the clinical trial in order to tell you what you think afterwards.”
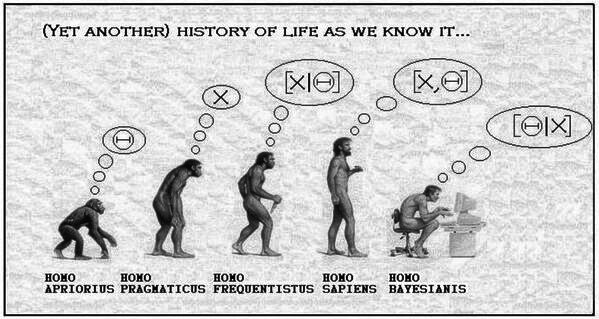
Now, look at Figure 8. What do the humans and pre-humans think if they see a congener with a sardonic smile. The ‘homo frequentisticus’ knows that killing humans have a sardonic smile (>95% sure), so he grabs his knife. The ‘homo sapiens’ knows there is some covariation between sardonic smile and killing, so he holds back. The ‘homo bayesianis’ calculates his chance of being killed if he sees that sardonic smile.
Homoeopathic prescription
In the information above you did not use two symptoms in establishing the diagnosis: the cough when entering a warm room from the cold and the fact that he holds his chest with his hands while coughing. These two symptoms match the homoeopathic medicine Bryonia (among others), because homoeopathic physicians in the past have noticed that these symptoms occur in patients responding well to Bryonia, and this experience is entered in the homoeopathic repertory. Probably you will ask some more questions and you might hear that the patient has much thirst for large quantities of cold drinks. The fact that the complaints started during a weather change from cold to warm weather (and this is common for these patients) makes you choose Bryonia as the medicine with the greatest chance of cure.
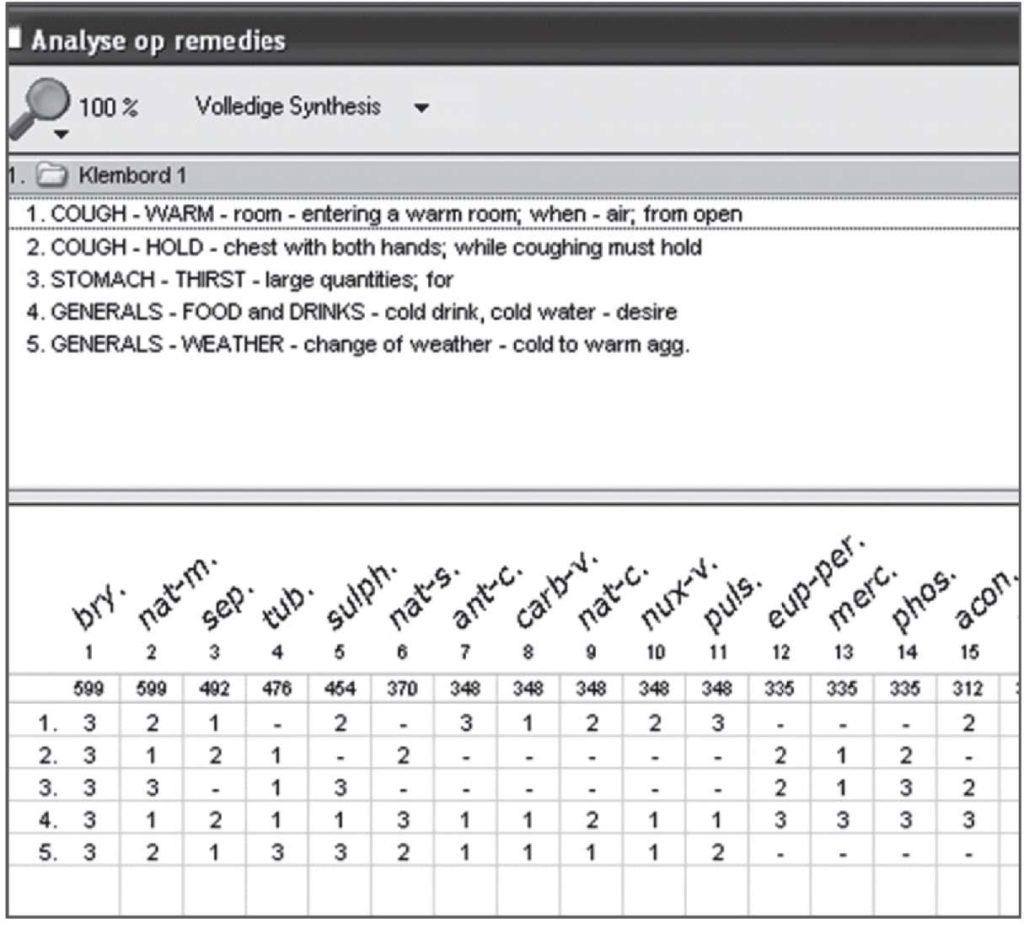
You can motivate your choice of homoeopathic medicine and make a graph of all eligible medicines like Figure 9. Homoeopathic doctors call this selection of medicines the homoeopathic (differential) diagnosis. However, this is not a diagnosis but a prognosis which medicine has the greatest chance to cure.
The statistics
In the diagnostic process, and also in the homoeopathic diagnosis – or rather prognosis – we saw growing confidence in the diagnosis and the prognosis by adding symptoms and signs. This confidence can be expressed as the estimated chance of a specific diagnosis or the estimated chance that a specific medicine will work. We can put these two processes beside each other in a table, like Table 8. We will explain this in the next chapter ‘Predicting the future and Bayes’ theorem’.
Table 8: Comparison of the conventional diagnostic process and the homoeopathic prognostic process.
| Diagnosis pneumonia | Chance | Prognosis Bryonia | Chance |
| Fever | 5% | Cough | 5% |
| Cough | 10% | < entering warm room | 20% |
| Rapid breathing | 30% | Hold chest while coughing | 40% |
| Dyspnoea | 50% | Thirst large quantities | 50% |
| Auscultation | 70% | Desire cold drinks | 60% |
| CRP + | 80% | Change from cold to warm w. | 70% |
The percentages shown in Table 8 are estimates made by experienced homoeopathic doctors. Doctors are working this way in diagnosis for centuries and ‘hard’ evidence like radiography of the chest shows that they are often right. The same goes for the homoeopathic diagnosis/prognosis. However, can this process be improved?
About the homoeopathic prognosis: in Figure 9 the medicine Natrium muriaticum (Nat-m) is mentioned for the symptom ‘Holds his chest with his hands while coughing’. I (LR) work with homoeopathy for >35 years and I have seen this symptom often. In my opinion, it is a reliable indication for Bryonia, but the symptom failed me at least once when prescribing Nat-m on this symptom (among other symptoms).
Useful research
To know if the symptom ‘Holds his chest with his hands while coughing’ is a reliable indication for Natrium muriaticum we can do research by checking this symptom in every new patient with cough. Then we treat the patient and collect the results after hundreds of patients. Now suppose that we see the following result after 400 patients with cough: the symptom occurred in 40 patients, 20 of these responded well to Bryonia, 1 to Nat-m and 19 to other medicines. The total number of successful prescriptions of Bryonia and Nat-m was 40 for both medicines. Therefore, the prevalence of the symptom ‘Holds his chest with his hands while coughing’ was 20/40=50% in the patient population responding well to Bryonia and 1/40=2.5% in the population responding well to Nat-m. So, the prevalence of this symptom is much higher (50% versus 2.5%) in the Bryonia population than in the Nat-m population. The comparison of this hypothetical comparison looks like Table 9.
Table 9: Prevalence of the symptom ‘Holds his chest with his hands while coughing’ in various populations
| Bryonia | Nat-m | All | |
| ‘Hands’ symptom | 20 | 1 | 40 |
| Total number | 40 | 40 | 400 |
| Prevalence | 50% | 2.5% | 10% |
We know that Nat-m is one of the most prescribed medicines, but it will not be prescribed in many cough cases. Therefore we estimate that it is in this group as many times prescribed as Bryonia. Now we see why Nat-m is in the repertory-rubric ‘Holds his chest with his hands while coughing’. In the system of the repertory, a medicine is added to a symptom-rubric if it occurred in a ‘cured’ patient. Intuitively we feel that frequently used medicines are over-represented in many repertories- rubrics. If we look at prevalence we can understand why, half of the patients responding well to Bryonia had the symptom, clearly more than the 10% in the whole population, and in the Nat-m population the symptom occurs less than in the whole population. Intuitively we understand that a symptom should occur more than average in a specific medicine-population to be included in the repertory-rubric.
Mind, here we used a hypothetical situation, this research has to be actually performed to see how good these estimates are. This example may overwhelm you a bit now, but rest assure, this way of handling statistics will be explained step-by-step in this book.
Conclusion
To do research that is really relevant for the patient we should focus on the patient’s basic questions “What’s wrong with me?” and “Will this medicine work for me?” These questions are about chances related to the patient in front of you. Diagnosis and prognosis research will give such answers, effectiveness research not because it relates to a comparison with placebo and an average effect in an average patient. We should give more emphasis to prognosis research using the same methods as in diagnosis research. In this respect, every case can be valuable if properly recorded. The combined information of all cases in the past tells us what to do in the future helping the individual patient.
Reference: Fundamentals of Statistics & Clinical Research in Homoeopathy by Lex Rutten & Martine